Authors
Ngoc L. VanHorn, MD1, Mary E Jones, BA, CHSOS, CHSE2, Jeanne Carey, MEd, RN, CHSE-
A2, Krystle K. Campbell, DHA, MS, CHSE, FACHDM2
1University of Texas Southwestern Medical School, Dallas, TX
2University of Texas Southwestern Simulation Technology & Education Center, Dallas, TX
Conflict of Interest Statement
The authors declare no conflict of interest.
Corresponding Author
Brief Description
Simulation-based medical education (SBME) has been shown to be a valuable adjunct to traditional didactic instruction and clinical exposure, affording trainees the opportunity to engage in medical decision-making and error analysis without endangering live patients. SBME facilitates the acquisition of procedural competencies, team coordination, effective communication, and comprehension of medical protocols within a controlled and psychologically safe setting. Nevertheless, the implementation of SBME with appropriate fidelity to meet a session’s objectives is constrained by the demand for multiple embedded participants (EP) to ensure optimal simulation outcomes. The aim of this manuscript is to present a case study in the creation of free digital avatars for use in scenario-based, multi-modal simulation activities. Use of digital avatars can reduce the need for human EPs, while maintaining the psychological and conceptual fidelity of the scenario.
Introduction
Simulation-based medical education (SBME) has witnessed a notable surge in prominence over the last two decades, becoming an indispensable component of medical education curricula across various training levels (McGaghie et al., 2016). Prospective trainees increasingly prioritize programs which integrate robust simulation curricula alongside traditional didactic instruction (Everson et al., 2020). SBME offers educators the opportunity to replicate complex clinical scenarios within a controlled environment (Frey-Vogel et al., 2022), serving as a viable substitute for direct patient encounters (Cheng et al., 2014). Extensive empirical evidence underscores SBME's efficacy as an instructional modality (Frey-Vogel et al., 2022). When implemented adeptly, SBME has demonstrated a capacity to attenuate medical errors and enhance patient safety (Lamé & Dixon-Woods, 2020). Moreover, SBME furnishes a secure platform for trainees to scrutinize genuine errors and refine procedural and communication protocols (Kava et al., 2017). The Accreditation Council for Graduate Medical Education has advocated vigorously for the integration of SBME into residency programs, endorsing a broad conception of SBME that encompasses diverse modalities such as standardized patients, objective structured clinical examinations, and task trainers, among others (Goolsarran et al., 2018).
SBME offers a plethora of significant advantages, yet its effective implementation necessitates considerable investments in terms of time, resources, and manpower (Acton et al., 2015; Ker et al., 2021; Zendejas et al., 2013). The number of embedded participants (EP) needed for simulation scenarios fluctuates depending on multiple factors such as the simulationist’s preferences and the need for inclusion to meet the defined learning objectives. An EP is an individual who is trained to play a role in a simulation encounter to help guide the scenario. The EP serves as an important resource for SBME, interacting with the learners and increasing engagement (Koca et al., 2023). The EP is often called upon to provide key information during the simulation activity. If the learner is going astray, the EP can help redirect the participant through the delivery of cues (Watts et al., 2021). Embedded participants increase the realism of the simulation activity. Portraying the role of another health care provider or family member adds to the environmental and psychological fidelity (Watts et al., 2021).
The EP is meant to be an adjunct and should not unduly exert influence on the learner’s behavior. However, EP performances can vary greatly if not properly trained, negatively impacting the learner experience (Watts et al., 2021). Hiring, training, and directing human role players as embedded participants requires resources of time and money (Koca et al., 2023). The creation and use of digital avatars can be more cost effective, while also alleviating the variability of performance among human EPs.
To address these challenges, we created and deployed simple, free custom digital avatars to reduce the demand for human volunteers as an EP. The aim of this manuscript is to show the step-by-step process of creating free digital avatars for use as EPs in scenario-based, multi-modal simulation activities. We hypothesized that digital avatars could reduce the need for additional volunteers to act as EPs while maintaining situational realism and psychological safety. This would most benefit novice simulationists and curriculum development specialists, as well as those conducting simulations with limited financial or human resources.
Use of Avatars in SBME
An effective simulation scenario often necessitates the engagement of multiple human participants beyond the simulationist. The multi-discipline nature of patient management parallels the complexity inherent in simulation aimed at replicating real-life situations (FreyVogel et al., 2022). However, achieving such fidelity is challenged by constraints such as limited faculty availability, scheduling intricacies, and familiarity with simulation instruction. The creation of digital avatars emerges as a pragmatic solution (Hatton, 2023).
Digital avatars can assume diverse roles essential to the realistic enactment of a scenario. Avatars can play the part of the parent, bedside nurse, other healthcare provider, social worker, chaplain, or other role necessary for a realistic scenario. Moreover, these avatars can be programmed to deliver both scenario-specific dialogues and general statements, thereby facilitating their utilization in subsequent simulations. Standardized digital avatars can be systematically amassed into a repository for integration into future simulation scenarios.
Avatars can be customized to embody varying genders, ages, ethnicities, and demographic profiles, incorporating accents or linguistic diversity to mirror the patient population or healthcare workforce of specific regions. Presenting diverse voices through simulations while encouraging self-reflection, are essential for reducing biases and microaggressions (Picketts et al., 2021). Avatars can be intentionally created to promote diversity and counter targeted recruitment of human role players (Picketts et al., 2021). These avatars can be placed in various environments, such as hospital wards, homes, or public places like concerts, making them useful and scalable for different types of simulations. They prove instrumental in navigating challenging patient interactions as well as assuming roles of actors in critical medical resuscitation scenarios.
A well-structured setup allows for versatile access to these avatars during scenario facilitation. They can be linked to QR codes for convenient retrieval via individual smart devices. Moreover, they are adaptable to be viewed remotely via various display mediums, including television screens, computers, or touchscreen tablets. Digital avatars are not limited to high fidelity scenarios. They can enhance tabletop scenarios, low-fidelity manikins, and simple standardized patient encounters by acting as patients and providing predetermined responses, thus improving the realism of the simulation (Howard, 2018).
Avatar development and facilitation
Our simple process allows for immediate creation and integration without requiring additional funding or stakeholder support. It is a good introduction for the technologically naïve to integrate new skills into their live-action simulation events.
Creation of free digital avatars
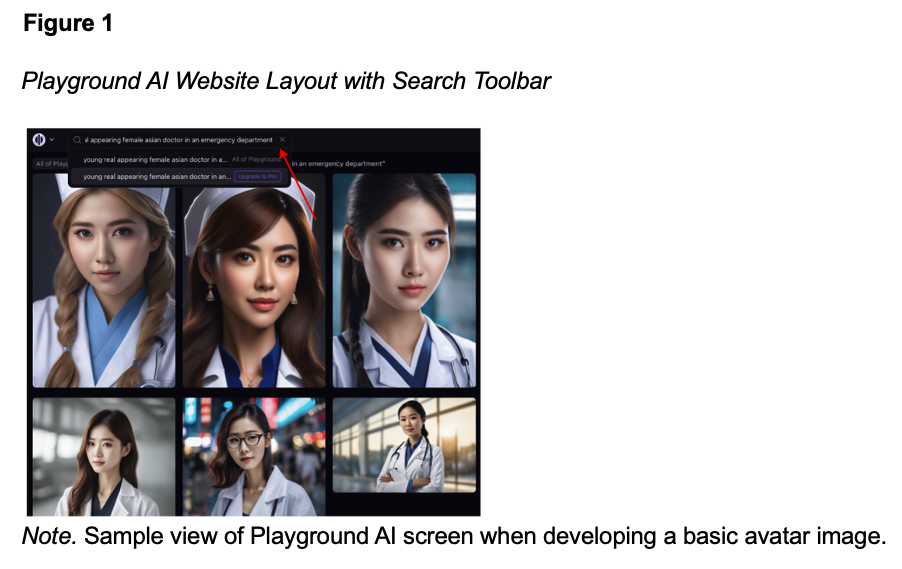
Part 1: Create the digital avatar image
2. Create an account.
3. In the top toolbar, enter a description of your desired image with as much specificity as possible. Consider the avatar’s age, race, image realism, dress, background environment, and other details such as props or identifying markers (e.g., stethoscope, tattoos, piercings, and profile vs. full body image) (Figure 1).
4. Download and save the digital avatar.
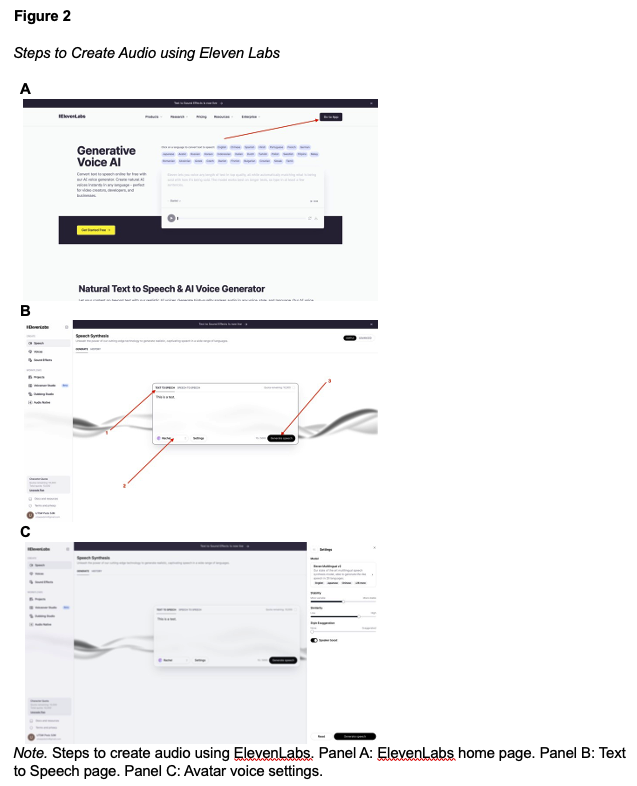
Part 2: Create the audio
2. Create an account.
3. Click “Go to App” in the upper right-hand corner (Figure 2A).
4. In the “Speech Synthesis” page, ensure “Text to Speech” is selected (Figure 2B, arrow 1). Type out your audio message.
5. Beneath the text box, click the “Rachel” drop down box to hear a sample of different voices. Choose your desired avatar voice from the list (Figure 2B, arrow 2).
6. To the right of the “Rachel” drop down box, click “Settings”. A right-hand box will appear to select the spoken language of the avatar (Figure 2C).
7. Once you have typed your audio message and adjusted the settings, select “Generate” to create the audio file (Figure 2B, arrow 3).
8. Download and save the audio file.
Part 3: Combine image and audio
2. Establish an account associated with a free trial period.
3. Click “Create Video” (Figure 3A).
4. Click “Add” to upload the avatar created from Playground AI (Figure 3B).
5. Ensure your created image is selected. Click “Audio” to upload the voice clip created from Eleven Labs (Figure 3C).
6. Click “Generate Video” and download the finalized avatar (Figure 3D).
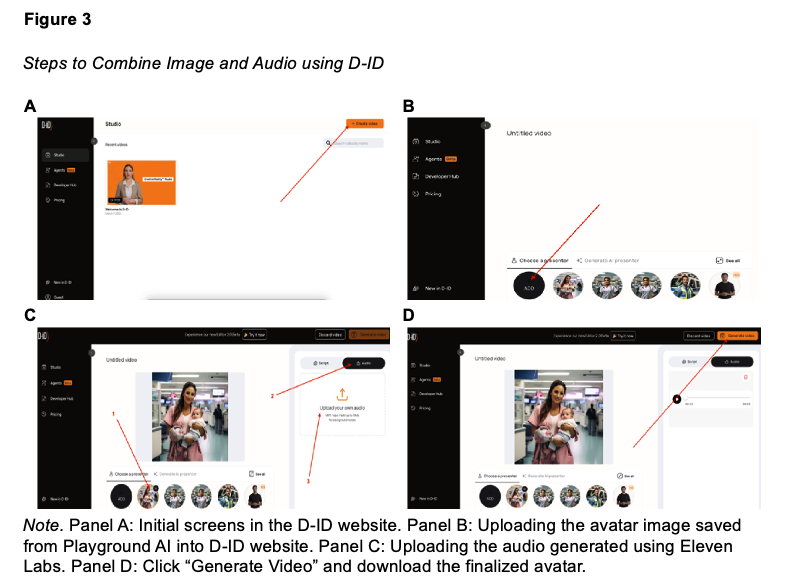
Steps to Combine Image and Audio using D-ID
If the dialogue or image needs to be edited, an entirely new avatar image will need to be created. The generated images can be reused with different dialogue to maintain continuity throughout a scenario.
Discussion
We have implemented these custom digital avatars in our live-action simulations with pediatric residents, pediatric pharmacy residents, and pediatric emergency medicine fellows with improving execution. They have been used in scenarios such as multi-injury trauma, betablocker ingestion, cardiac arrest, and multi-system inflammatory syndrome in children. Most of our avatars play the EP role of the caregiver or other healthcare provider (i.e., bedside nurse or paramedic). In these roles, the avatars provide the scenario prompt, the patient’s history of present illness, or ‘lifesaving’ interventions when the scenario goes awry. The avatars are displayed to the entire team via a television screen or to individual participants through a QR code accessed on smart devices.
We have received verbal feedback that participants enjoy procuring information from “people” they do not know. Participants also reported that it mimics real-life history taking and data gathering. Using avatars also standardizes the experience across learner groups, ensuring all trainees receive a similar learning experience.
In the future, we hope to have multiple displays to represent an individual avatar. This will more accurately simulate a hospital environment by incorporating multiple embedded participants simultaneously. This would enhance the simulation by replicating various environmental noises.
Conclusion
The creation of digital avatars is a promising technology accessible to simulationists. This technology has the potential to address barriers to SBME execution highlighted in the literature. This includes lessening the burden to secure adequate human volunteers to ensure psychological and conceptual fidelity. Digital avatars also serve to expand representation and diversity of embedded participants. Avatars offer an innovative solution for both experienced and novice simulationists to uphold fidelity and psychological safety. Here, we offer a simple and free method to create digital avatars that can reflect diverse patient populations or healthcare workforces. This process enables simulationists to seamlessly integrate digital avatars into scenario-based, multi-modal simulation activities without requiring additional technological, financial, or human resources.