AUTHORS
Merryl Lopido, BS, CHSOS1; Allyson Molzahn, BS1; Dave Biffar, MS, CHSOS-A, FSSH1; Allan Hamilton, MD, FACS1,2; Kate Hughes, DO3
1 Arizona Simulation Technology and Education Center, Health Sciences, University of Arizona, Tucson, AZ
2 Department of Surgery, University of Arizona, Tucson, AZ
3 Department of Emergency Medicine, University of Arizona, Tucson, AZ
Corresponding Author
Merryl Lopido, merryl07@arizona.edu
SUMMARY
Ultrasound-guided peripheral intravenous access is a valuable technique in patients with difficult venous access, and proficiency with this skill is essential for healthcare providers across a range of clinical settings. There are several commercially available models for ultrasound-guided IV placement; however, they tend to be costly with limited reusability. We sought to develop an advanced USIV model featuring anatomically realistic vessel paths and a high-fidelity ultrasound image which learners can use to practice discriminating between artery and vein.
The model was made using ballistics gel to simulate soft tissue, a 3D-printed mold and base, and fluid circuit to simulate vessels. We completed a preliminary evaluation of the model using feedback from Anesthesia residents with clinical experience placing ultrasound-guided IVs. Based on this feedback, we revised the model and completed a formal evaluation with subject matter experts. Most experts rated each aspect of the model as at least somewhat realistic or better, including the vascular anatomy on ultrasound, tissue quality, and overall realism. They reported the model could be improved by adding surrounding structures, such as nerves and muscles, as well as improving the simulated arm shape. Here, we present a cost-effective, reusable ultrasound-guided IV training model along with construction instructions and expert evaluation of model realism.
INTRODUCTION
Establishing peripheral intravenous (IV) access is a fundamental skill for all healthcare professionals, facilitating medical diagnosis and treatment. Usually, this can be achieved by visualization and vessel palpation. However, intravenous access can be difficult to establish in the setting of obesity, intravenous drug abuse, hypovolemia and previous difficult IV access. In these situations, ultrasound guidance can facilitate peripheral IV access while avoiding multiple painful attempts and waste of additional supplies (Adhikari et al., 2015). Importantly, in high-acuity emergent settings where rapid IV access is crucial, adequate training of healthcare professionals performing the procedure can prevent unnecessary delays in patient care (Edwards & Jones, 2017). Given the importance and prevalence of establishing IV access, practicing the procedure on a realistic model is crucial to developing and honing this skill.
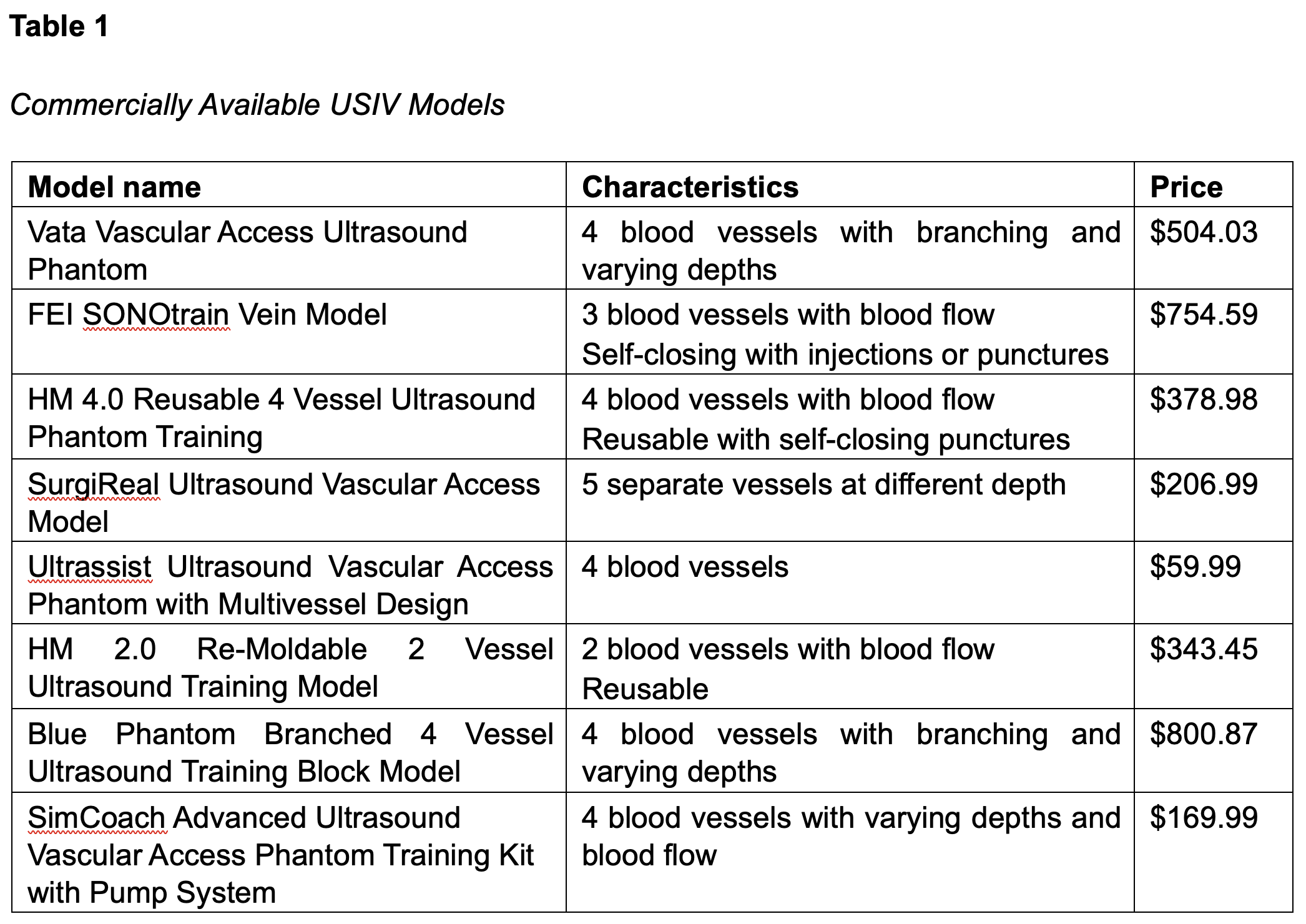
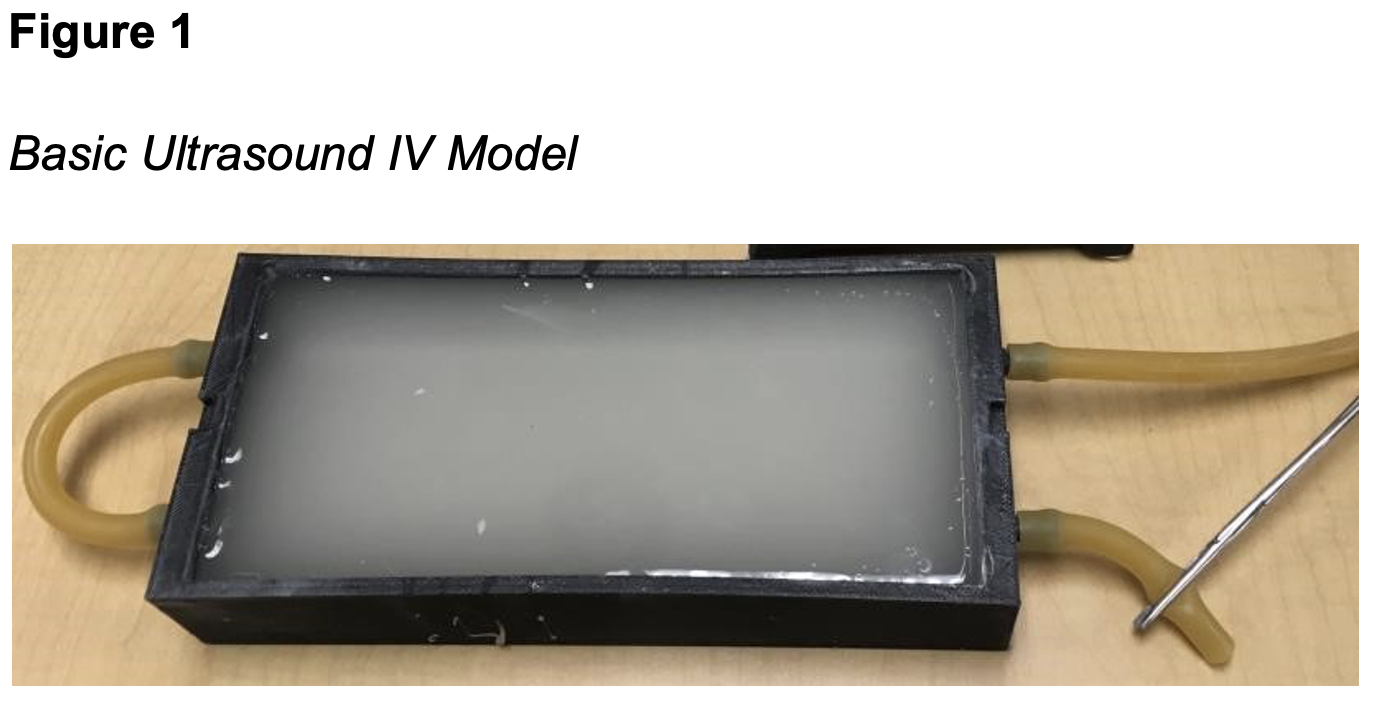
There are several manikins, phantoms and models available for teaching ultrasound-guided IV (USIV) placement. The commercially available models tend to be costly with limited reusability (Table 1). At our simulation center, we previously used a basic USIV model (Figure 1). However, a collaboration with the Emergency Medicine Ultrasound Fellowship program highlighted that the simple, straight vessels of our basic model limited its ability to develop skills of experienced learners. We sought to develop an advanced USIV model featuring anatomically realistic vessel paths and a high-fidelity ultrasound image that challenged learners to discriminate between artery and vein. We sought subject matter expert feedback to evaluate the realism of the vessel anatomy and ultrasound image, and the educational value of the model.
METHODS
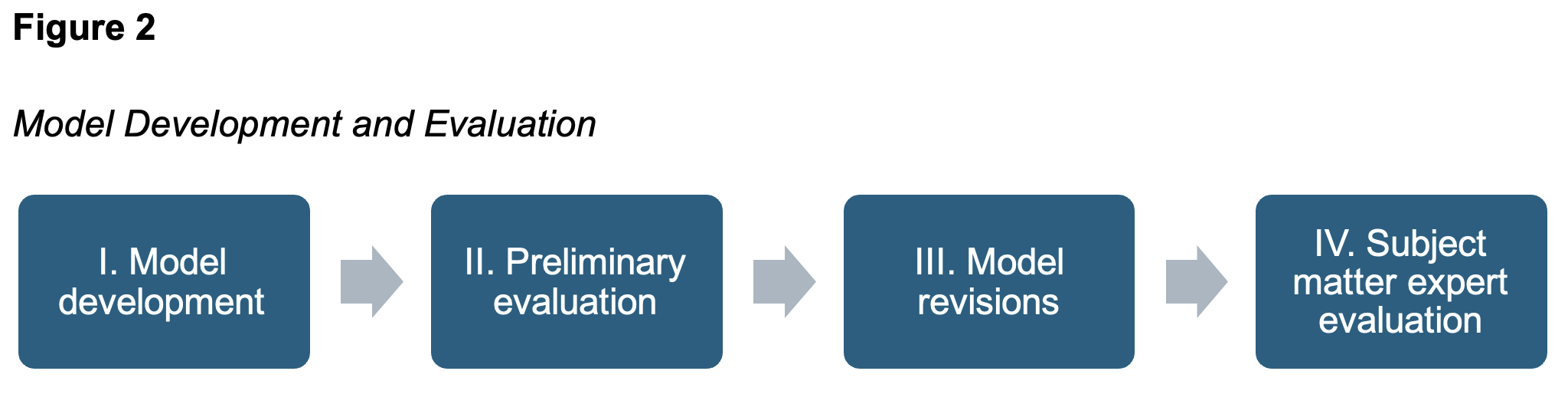
This is a qualitative study to assess a newly developed ultrasound-guided IV insertion model conducted in four phases: model development, preliminary evaluation, model revisions, and subject matter expert evaluation. During model development, the research team collaborated with an Emergency Medicine Ultrasound Fellow to create a clinically accurate model. Following development, a preliminary evaluation was conducted with anesthesia residents, gathering feedback from trainees familiar with ultrasound-guided IV placement. This feedback informed iterative improvements to the model’s design and functionality. Finally, formal evaluation phase was conducted, engaging subject matter experts from Emergency Medicine where USIV is commonly utilized. The development and evaluation process is summarized in Figure 2.
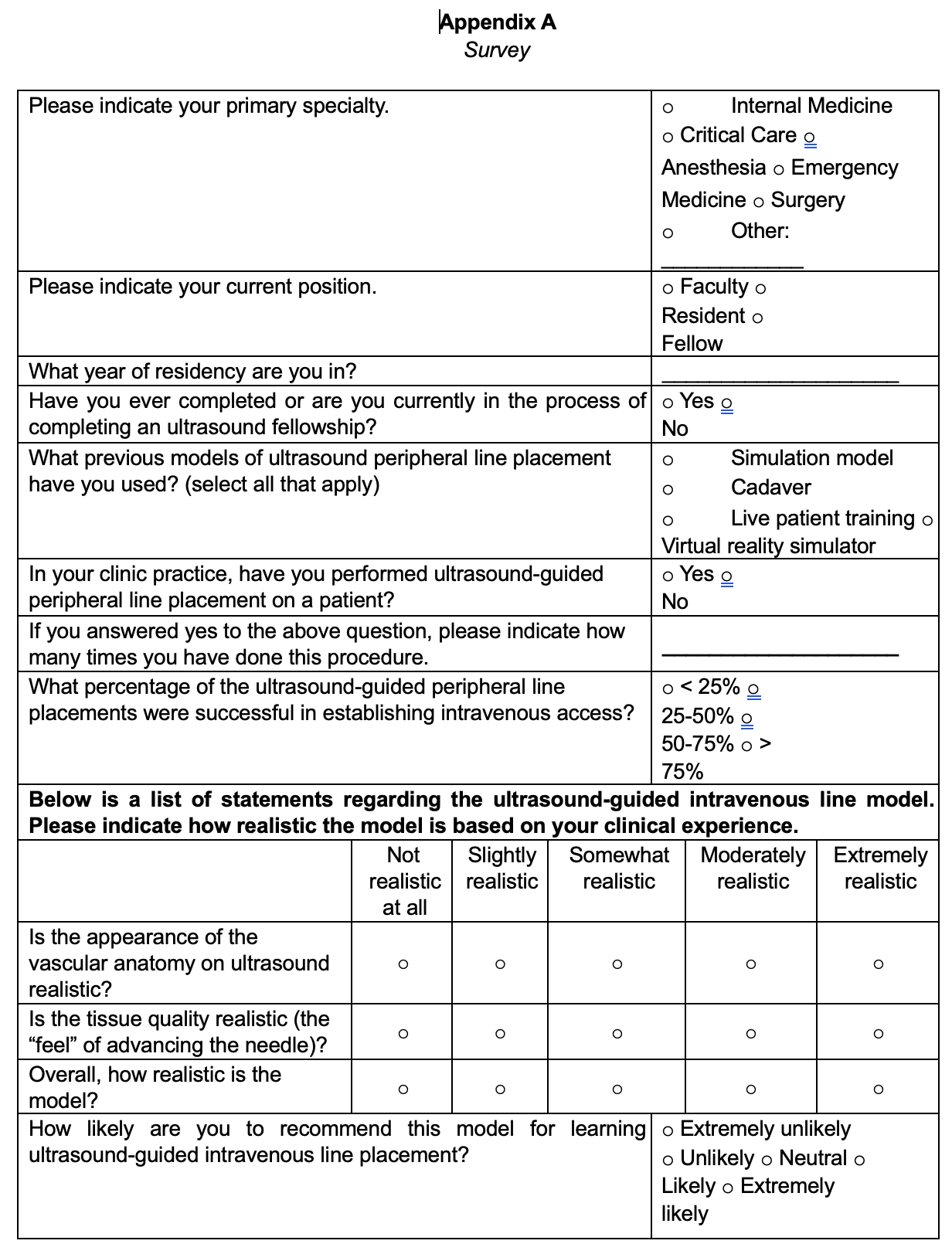
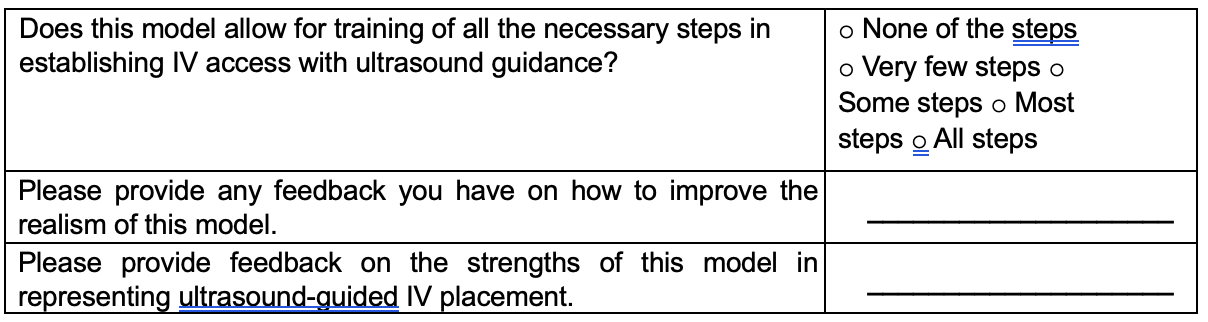
We completed the study within a dedicated research space at the Arizona Simulation Technology and Education Center (ASTEC). The space included the advanced USIV model and supplies for performing the procedure. The Institutional Review Board of the University of Arizona approved this study on August 29, 2024 (ID 11008100). Informed consent for inclusion in this research study was obtained electronically prior to enrollment in the study. For both evaluation phases, we collected demographic information on each participant’s specialty, training level, experience, and success with USIV placement. Participants then completed a survey created by the research team asking them to rate image quality, tissue, haptics, overall realism, and utility as a training tool. The survey also included two free-response questions: one on suggestions for improving the model and another on its strengths (Appendix A).
RESULTS
The development and evaluation of the ultrasound-guided IV model occurred in four phases: model development, preliminary evaluation, model revision, and subject matter expert evaluation. Results from each phase are presented below.
I. Model Development
As discussed above, ultrasound-guided IV placement is a commonly performed procedure, especially in Emergency Medicine and Ultrasound training. Although our previous model had adequate appearance under ultrasound, the vessels were shallow and followed a linear path. The model base did not resemble an arm in shape or orientation. To create a higher fidelity model for practicing ultrasound-guided IV placement, we sought to accurately replicate vascular anatomy under ultrasound imaging and deliver realistic needle insertion haptics, bridging the gap between simulation and clinical practice.
Model Design Considerations
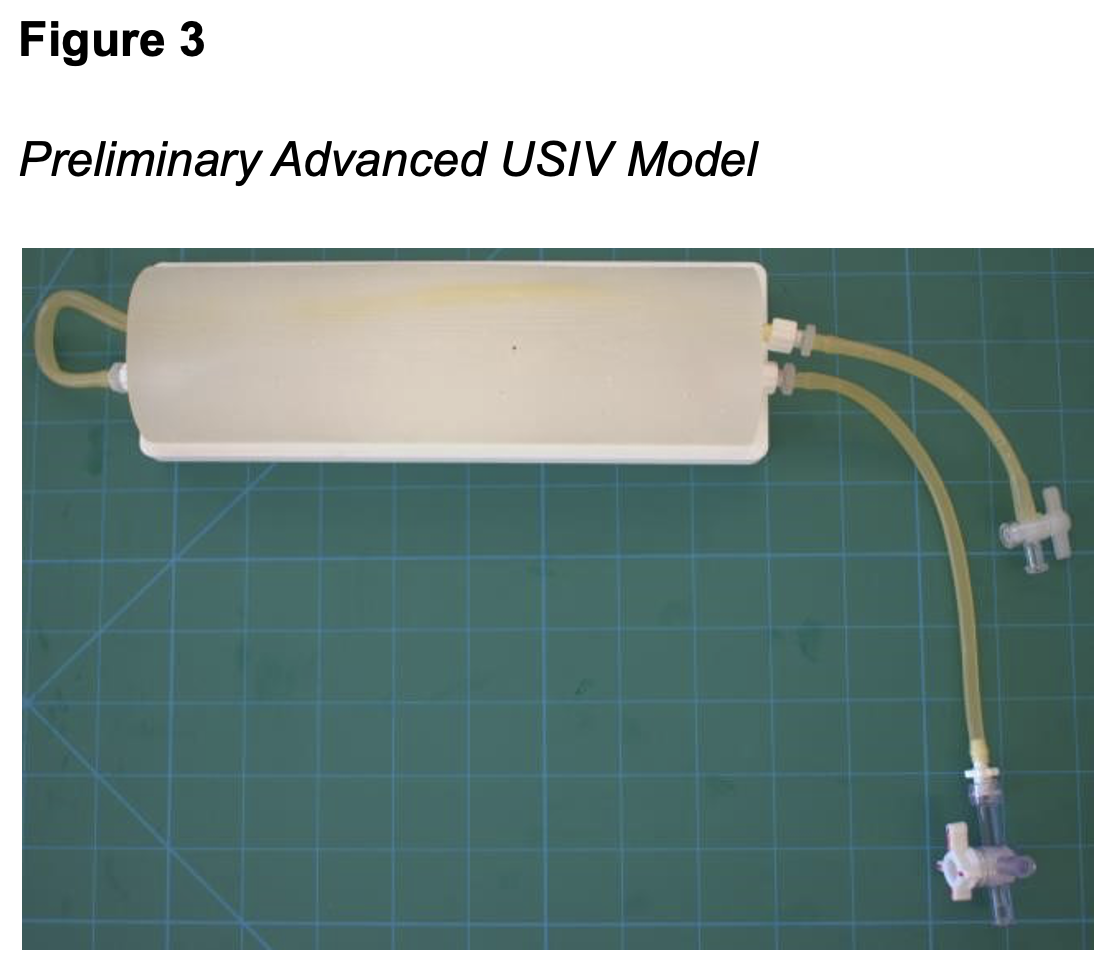
Full written and video instructions for the final model can be found in Appendix B and are publicly available the ASTEC Makerspace page (https://astec.arizona.edu/facilitymakerspace/makerspace). In brief, the model base was 3D printed. Ballistics gel was used to simulate both the haptics and sonographic appearance of involved structures as it provides a realistic image of human tissue with ultrasound imaging. During model making, a stylet was inserted into the silicone tubing to simulate the irregular path and varying depth of the vessels. The artery is differentiated from the vein by the presence of latex tubing simulating a thick walled, incompressible artery. To simulate the vein, a negative space was created by removing the tubing. Using an IV bag and tubing to create a fluid circuit, the model provides a “flash” when the learner correctly placed the IV catheter in the vein. The model before revisions were made based on preliminary evaluation results is shown in Figure 3.
II. Preliminary Evaluation
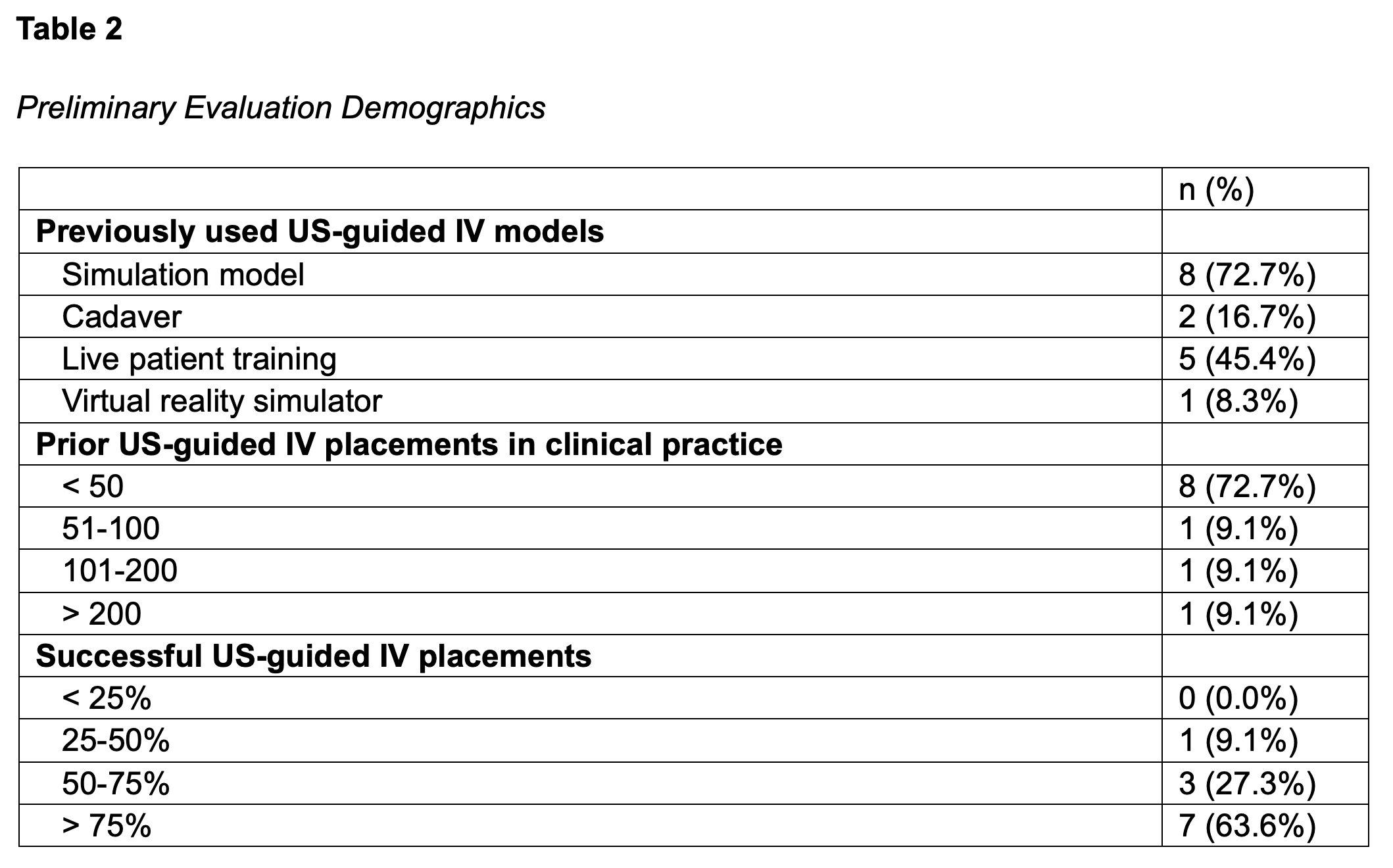
Following model development, we completed a preliminary evaluation phase with Anesthesia residents to gather feedback and make improvements to the model as needed. Anesthesia residents were recruited during a simulation session in their residency curriculum at ASTEC in October 2024. Eligible participants were Anesthesia residents present at the event with clinical experience performing USIV placement. In total, 12 participants were recruited, 11 of which were eligible (Table 2). Of the 11 eligible participants, 3 were in their second year of residency, 4 were in their third year, and 4 were in their fourth year. After informed consent, Anesthesia residents were asked to use the model to complete ultrasound-guided IV placement and provide feedback.
Preliminary Evaluation Results
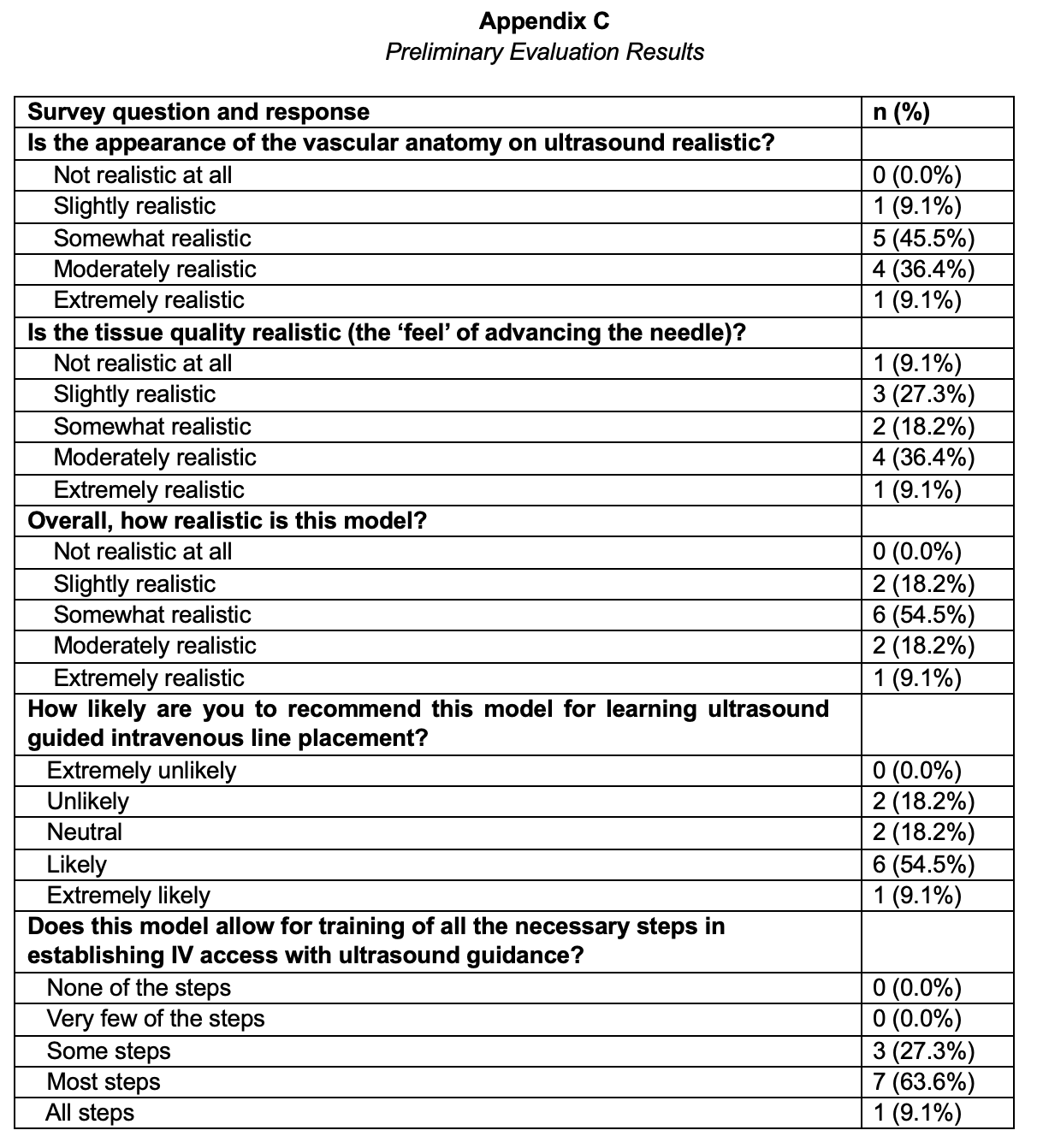
The results of the preliminary evaluation are shown in Appendix C. Most participants rated each aspect of the model as at least somewhat realistic or better, including the vascular anatomy on ultrasound (90.9%), tissue quality (73.6%), and overall realism (81.8%). Regarding its usefulness for learning ultrasound-guided IV line placement, 63.6% were "likely" or "extremely likely" to recommend the model, while 36.4% were neutral or unlikely to recommend it. When evaluating whether the model allowed for training the necessary steps in establishing IV access with ultrasound guidance, 8 (72.7%) participants indicated it included "most" or "all" steps, while 3 (27.3%) reported it included "some steps."
To improve the model, participants recommended adding a flash to confirm the needle was in the correct location (n = 5), making the vascular anatomy more superficial (n = 2), adding tortuous veins (n = 1), and modifying the tissue to be more pliable (n = 3). Participants identified the
appearance of anatomy on ultrasound (n = 5), tissue resistance (n = 2) and inclusion of deep veins (n = 1) as strengths of the model. Two respondents reported the model would be good for novice learners practicing the procedure.
III. Model Revisions
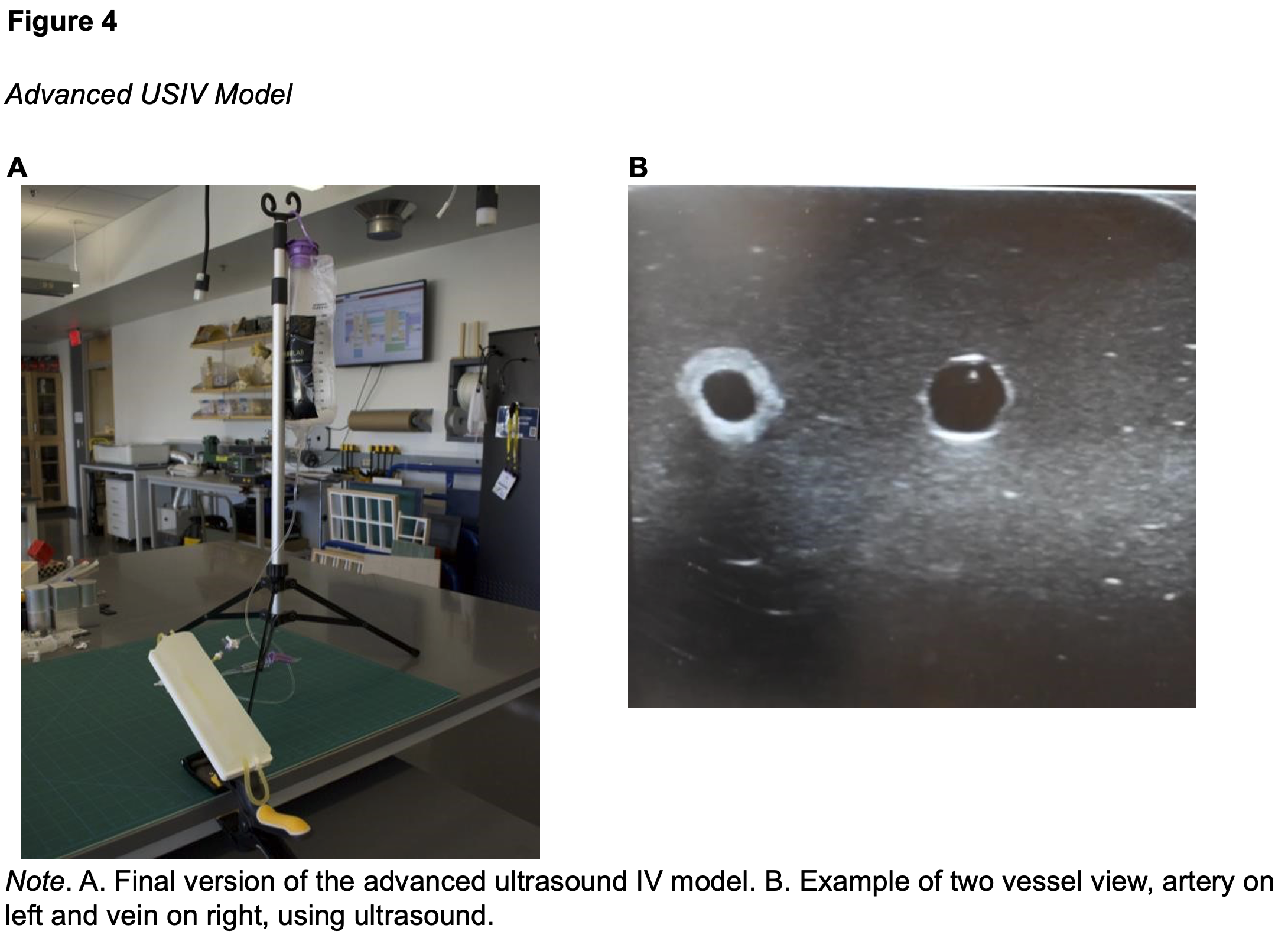
To address the feedback from the preliminary evaluation, we added internal silicone tubing to represent the vessels. Leaving the tubing in the model eliminated leaking to allow for enough pressure to provide a flash to confirm correct needle placement. By leaving the tubing in, the artery and vein can be differentiated by the thicker walled, less compressible tubing simulating an artery and thinner walled for vein. Silicone tubing was chosen over latex as it is more heat-resistant and not altered when exposed to the heat of the melted ballistics gel. Although several participants suggested making the tissue more pliable, the research team prioritized preserving the realistic ultrasound appearance of the ballistic gel. Because the model’s sonographic anatomy was consistently identified as one of its greatest strengths, we did not change the material.
In addition to the above changes, the research team noticed several participants struggled with the unsteady base of the model. To address this, a new base was designed to improve stability during learner operation. The updated model can be seen in Figure 4. Written and video instructions on how to make the model are provided elsewhere (Appendix B).
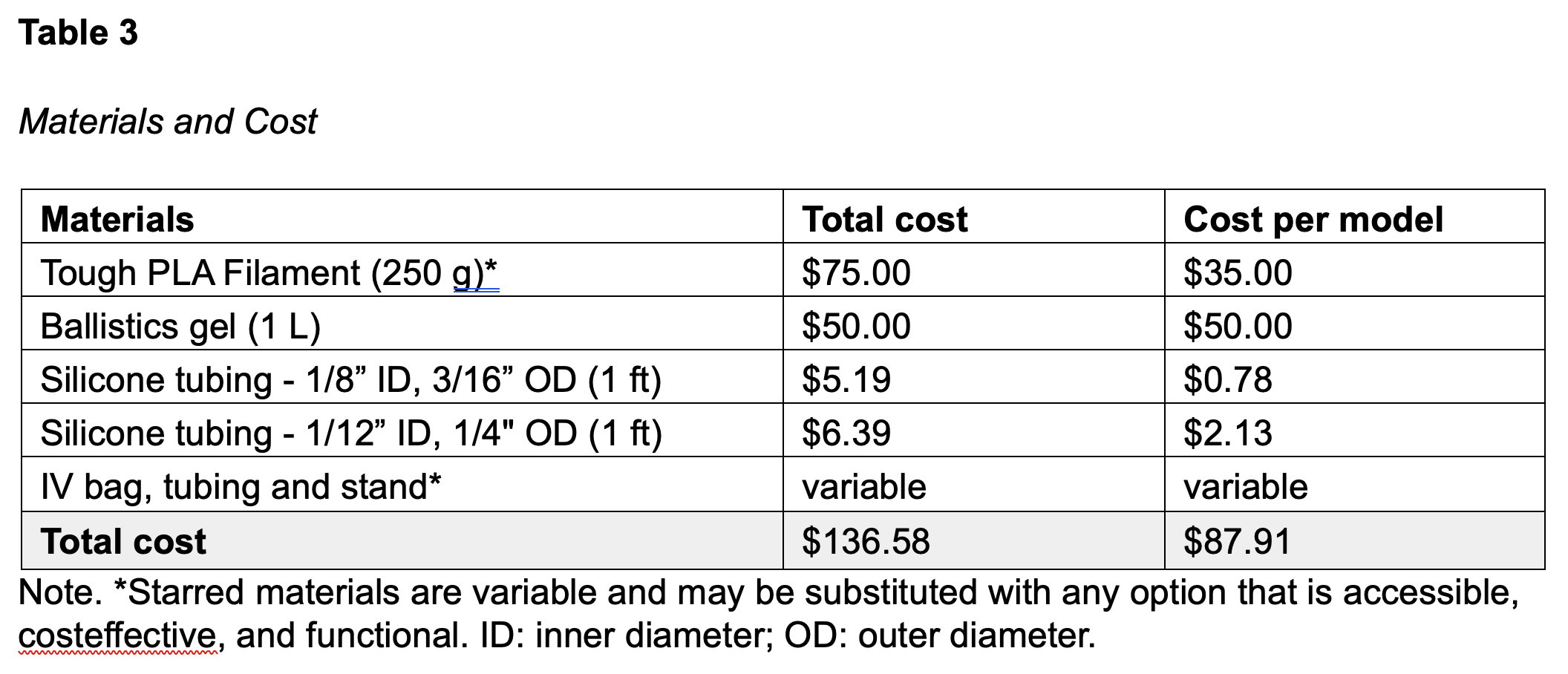
The materials and costs required to construct a single model are listed in Table 3. For our fluid circuit, we used an IV bag, tubing and stand already in our lab; however, any cost-effective and accessible alternative is suitable. Similarly, while we used a 3D-printed mold and base fabricated from tough PLA filament, any comparable container and stand can be substituted based on available resources.
IV. Subject Matter Expert Evaluation
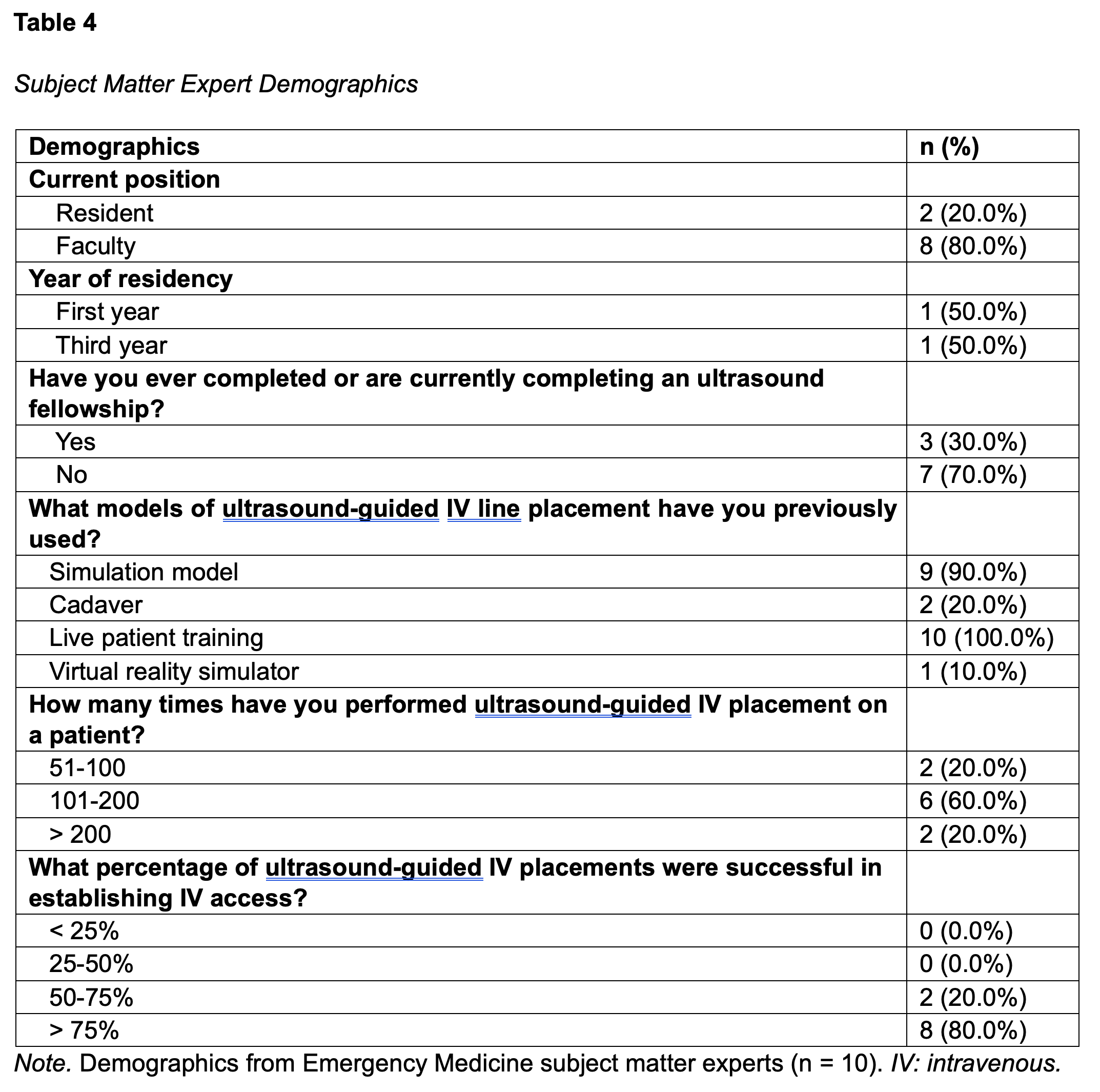
The research team recruited subject matter experts from the Emergency Medicine Airway Day at ASTEC in October 2025. Eligible participants included faculty and residents from Emergency Medicine who have clinical experience placing USIV. We defined subject matter experts as participants who have more than 50 prior USIV placements. This threshold is based off recommendations from the American College of Emergency Physicians and American Institute of Ultrasound in Medicine (American College of Emergency Physicians, 2023; American Institute of Ultrasound in Medicine, 2025). In total, of the 17 participants recruited, 10 qualified as subject matter experts. The participant demographics of the subject matter experts are shown in Table 4.
Subject Matter Expert Feedback
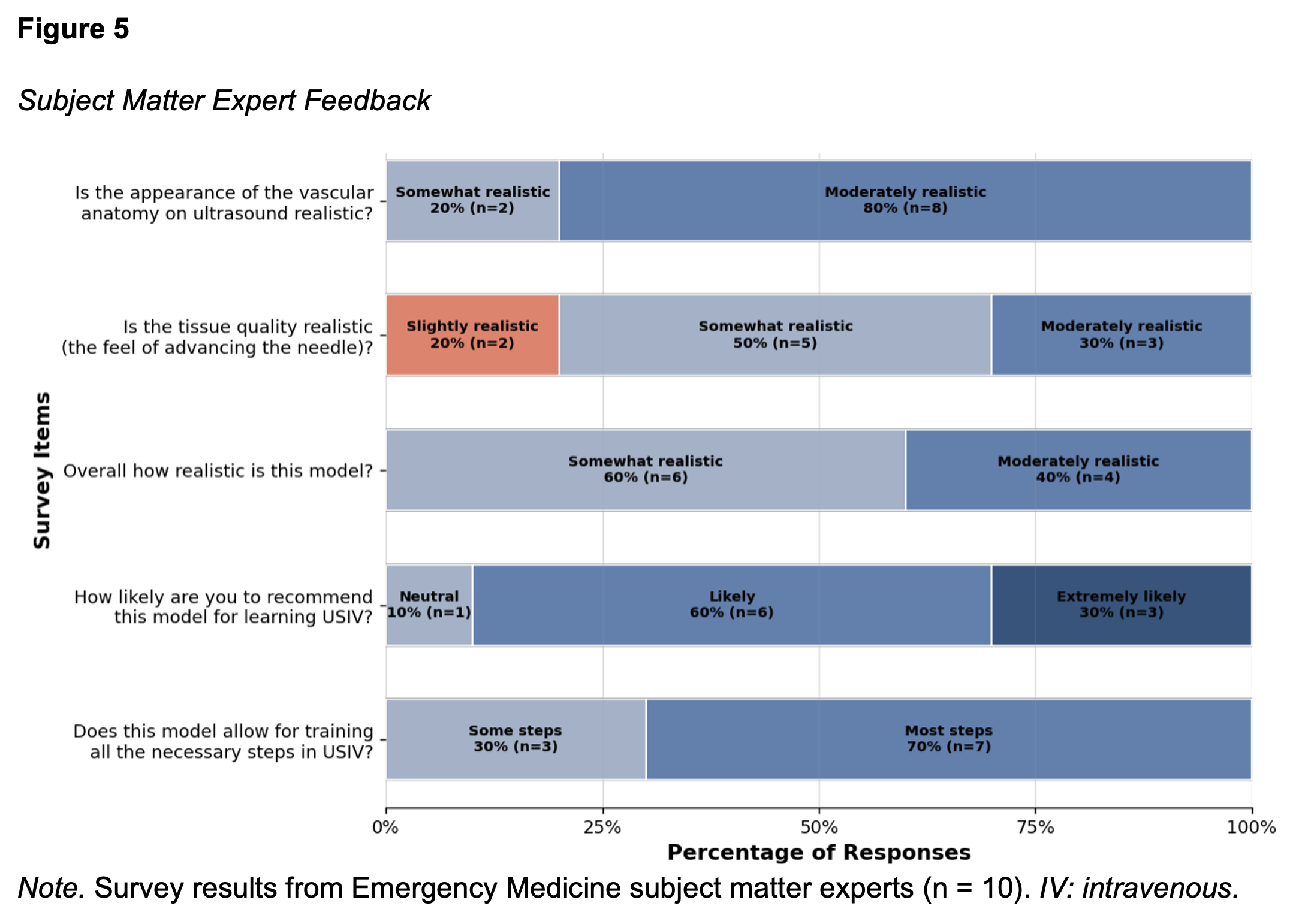
The survey results from subject matter experts are shown in Figure 5. Most experts rated each aspect of the model as at least somewhat realistic or better, including the vascular anatomy on ultrasound (100.0%), tissue quality (80.0%), and overall realism (100.0%). Regarding its usefulness for learning ultrasound-guided IV line placement, 90.0% were "likely" or "extremely likely" to recommend the model, while the remaining were neutral (10.0%). When evaluating whether the model allowed for training the necessary steps in establishing IV access with ultrasound guidance, 7 (70.0%) participants indicated it included "most" or "all" steps, while 3 (30.0%) reported it included "some steps."
The most common suggestion to improve the model was to make the vasculature more irregular by including branch points or placing them laterally (n = 5). Participants also recommended reducing air artifact (n = 3), adding surrounding structures such as muscles and nerves (n = 3), and improving the simulated arm shape by making it flatter, including antecubital space and space for a tourniquet (n = 3). There were also several suggestions on how to improve the vasculature (n = 3), such as making a pulsatile artery, adding fibrinous vessels for additional difficulty, and improving distinction between artery and veins. Participants identified the realistic resistance of the tissue (n = 5) and appearance of anatomy on ultrasound (n = 4) as strengths of the model. Two participants praised the model for its functionality and usability, noting that it does not leak and can be reused.
DISCUSSION
In this study, we developed a cost-effective, reusable model for advanced ultrasound-guided IV placement. Based on preliminary feedback, we modified the model to make vessel path more tortuous, provide a flash to confirm correct location, and stabilize the model base. Subject matter experts found the vascular anatomy under ultrasound and the model overall to be realistic. This finding supports the model’s potential usefulness as a training tool for learners practicing ultrasoundguided vascular access.
Although several experts also commented that the tissue was somewhat firmer than human tissue, most agreed the sonographic image was a major strength of the model. Because the ballistic gel provided highly realistic ultrasound visualization, we prioritized preserving this rather than modifying the current materials. In future iterations, we plan to trial a softer ballistic gel to determine whether tissue realism can be improved without sacrificing the ultrasound image quality.
Experts also provided additional suggestions to enhance realism, such as incorporating a superficial skin layer, adding red dye to fluid to resemble blood, and replacing the IV bag with a syringe for an easier set up. While these modifications were not implemented in the present version, they represent practical options that could be integrated depending on educational goals. This highlights the versatility of this model. It is designed to be easily customized and adapted to different educational objectives, such as teaching vessel localization, needle visualization, or catheter advancement.
For our model, the total cost of materials to create one model was approximately $87.91 USD. Although the model’s longevity has not been formally assessed, ballistics gel is well established to withstand multiple needle passes before degradation of ultrasound image quality (Ewald et al., 2018). Other commercially available models ranged in price from $59.99 to $800.87, with an average price of $402.39. When accounting for the reusability of both the ballistic gel and the model base, this approach is substantially less expensive than commercially available models.
LIMITATIONS
This study has several limitations. Our sample of subject matter experts were all Emergency Medicine physicians. While this is a common procedure utilized in Emergency Medicine, especially as part of the training for ultrasound fellowship, the model would be strengthened by feedback from experts in various specialties. Additionally, this study does not assess the validity of this model and its effectiveness in improving skills associated with ultrasound-guided IV placement. The durability of the model has not been formally tested, and future studies are needed to determine the number of uses or needle passes possible before remelting of the ballistic gel is required to maintain ultrasound image quality. Future studies will aim to gather feedback from experts in different specialties, assess clinical improvement with model use, and monitor the model’s longevity after several uses.
CONCLUSIONS
This study demonstrates a low-cost, modifiable approach to developing a realistic ultrasoundguided IV model suitable for advanced training. Future versions of this model will focus on improving tactile feedback and testing the model’s effectiveness in improving learner skill acquisition.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Please cite this article as: Lopido, M., Molzahn, A., Biffar, D., Hamilton, A., & Hughes, K. (2026). Development of an advanced ultrasound intravenous line trainer. Simulation Technology & Operations Resource Magazine, 5(2), 1-12. ISSN: 3070-3506.
REFERENCES
Adhikari, S., Schmier, C., & Marx, J. (2015). Focused simulation training: Emergency department nurses’ confidence and comfort level in performing Ultrasound- Guided vascular access. The Journal of Vascular Access, 16(6), 515–520. https://doi.org/10.5301/jva.5000436
American College of Emergency Physicians. (2023, April 1). Ultrasound guidelines: Emergency, point-of-care, and clinical ultrasound guidelines in medicine. https://www.acep.org/siteassets/new-pdfs/policy-statements/ultrasound-guidelines-emergency-point-of-care-and-clinical-ultrasound-guidelines-in-medicine.pdf
American Institute of Ultrasound in Medicine. (2025, March 29). Training guidelines for physicians who evaluate and interpret diagnostic ultrasound examinations. https://www.aium.org/resources/training-guidelines/view/training-guidelines-for-physicians-who-evaluate-and-interpret-diagnostic-ultrasound-examinations
Edwards, C., & Jones, J. (2017). Development and implementation of an Ultrasound- Guided Peripheral Intravenous Catheter program for emergency nurses. Journal of Emergency Nursing, 44(1), 33–36. https://doi.org/10.1016/j.jen.2017.07.009
Ewald, J. M., Cheng, J. W., Engelhart, S. M., Wilkinson, M. C., Hajiha, M., Wagner, H., & Baldwin, D. D. (2018). A realistic, durable, and low-cost training model for percutaneous renal access using ballistic gelatin. Turkish Journal of Urology, 45(1), 31– 36. https://doi.org/10.5152/tud.2018.43569
Appendix B
Full written instructions and video
Written instructions: https://astec.arizona.edu/sites/default/files/2026-05/US-IV-Advanced-Instructions.pdf
Video: https://arizona.app.box.com/s/xp83j2ygc3wbyqusgq0lvphcn658g0f9