Authors
Katy Howarth, BSN, RN1, Marco Castelo, MSN, RN2, Sumit Singh, MD3
1National TeleCritical Care Program, Veterans Health Administration, Minneapolis, MN
2Department of Research, Innovation and Development, Greater Los Angeles Veterans Affairs Medical Center, West Los Angeles, CA
3Department of Surgical Intensive Care and Anesthesiology, Greater Los Angeles Veterans Affairs Medical Center, West Los Angeles, CA
Conflict of Interest Statement
The authors of this manuscript declare no conflicts of interest.
Corresponding Author
Katy Howarth, BSN, RN, National TeleCritical Care Program, Veterans Health Administration, Minneapolis, MN
(Email: Katy.Howarth@va.gov)
Introduction
The Veterans Affairs (VA) National TeleCritical Care (NTCC) Program is the world’s largest single TeleCritical Care service. It is designed to provide critical care expertise around the clock to over 70,000 Veterans annually. Leveraging advanced telehealth technologies and computer-enhanced algorithms, NTCC aims to enhance patient care outcomes through continuous support and collaboration with bedside clinical teams across 84 facilities and more than 1,200 Intensive Care Unit (ICU) beds.
A vital component of this program is the integration of TeleCritical Care simulation training, which is a pioneering initiative that employs high-fidelity simulation to promote a culture of safety and continuous improvement aligned with High- Reliability Organization (HRO) principles.
Objectives
- Describe the NTCC Program and its integration of TeleCritical Care simulation training.
- Illustrate how NTCC enhances patient care outcomes through interprofessional simulation training.
- Examine how NTCC Interprofessional Education (IPE) promotes a culture of safety and continuous improvement aligned with HRO principles.
About the VA National TeleCritical Care (NTCC) Program
Overview
The NTCC Program provides 24/7/365 critical care expertise to VA facilities, ensuring continuous patient monitoring and intervention. Currently, it covers 84 facilities with over 1,200 ICU beds, and an additional 14 facilities with 400 ICU beds are projected for future inclusion. The program supports the care of 70,000+ Veterans annually, with a daily average of 600-700 patients. This extensive network ensures that Veterans receive timely and high-quality critical care across the VA enterprise.
Technological Integration
NTCC employs advanced technologies, including real-time data access from electronic health records, imaging systems, waveforms, and clinical information systems, integrated through an enterprise telehealth software program. This setup allows continuous transmission and analysis of patient data using sophisticated algorithms, enabling the identification of at-risk patients and timely resource allocation for optimal care. The seamless integration of these technologies ensures that critical care teams have the most accurate and up-to-date information, facilitating better clinical decisions and outcomes.
Workforce
The NTCC team comprises board-certified critical care providers from various specialties and critical care nurses with diverse backgrounds such as trauma, cardiology, neurology, and military. The average critical care experience is 17 years for physicians and 13 years for nurses. This team of critical care experts brings a wealth of knowledge and experiences, ensuring high standards of care and fostering a collaborative environment that benefits both patients and staff.
NTCC Operational Divisions
The East and West divisions’ expansive network allows NTCC to provide extensive support and coverage ensuring that critical care resources are always available to 84 geographically dispersed VA facilities. This ensures consistent, timely access to state-of-the-art intensive care for all acutely ill Veterans whenever critical care services are required. The West Division is headquartered in Minneapolis, MN and oversees 42 VA facilities. This includes six NTCC hubs in Chicago, Iowa City, Garland, Las Vegas, Los Angeles, and Minneapolis. The East Division is headquartered in Cincinnati, OH and oversees 42 VA sites. This includes five NTCC hubs located in Ann Arbor, Atlanta, Baltimore, Cincinnati, and Orlando.
NTCC Roles and Interventions
The NTCC program delineates specific roles for its providers and nurses, ensuring a clear and efficient workflow that enhances patient outcomes. These roles are critical in ensuring that the NTCC program can effectively support bedside teams, offering expertise and guidance that can make a significant difference in patient outcomes.
NTCC Provider Role
- Writing orders
- Guidance during emergencies
- Critical care consultation
- Ventilator and sedation management
- ICU admission staffing during off-tour hours
NTCC Nurse Role
- Proactive alerts to hospital staff based on patient changes
- Safety risk and injury mitigation
- Peer-coaching
- Assistance during emergencies
- Routine rounding
TeleCritical Care Simulation Training
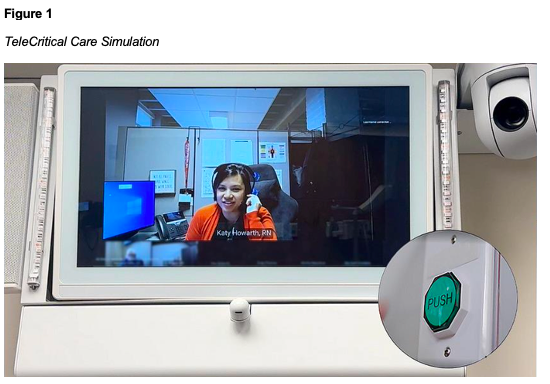
TeleCritical Care simulation was pioneered at the VA Greater Los Angeles Healthcare System, an academic-affiliated facility that provides simulation training for new cohorts starting their ICU rotation. These simulations utilize bi-directional telecommunication to conduct high-fidelity simulation scenarios focused on critical care and emergency response that are aligned with the standards of the Society for Simulation in Healthcare and the International Nursing Association of Clinical Simulation (Figure 1). The pioneering efforts at this facility have set a benchmark for other VA facilities, demonstrating the effectiveness of TeleCritical Care simulation in improving healthcare practices.
Outcomes of TeleCritical Care Simulation
Increased Utilization
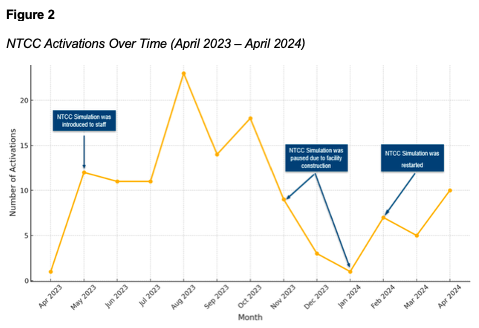
The following table illustrates the number of NTCC emergency activations since the commencement of simulation training in April 2023, see Figure 2. The number of activations increased during months simulation training occurred and decreased when simulation training was paused due to construction (November to February). The data reflects growing utilization and effectiveness of NTCC services, demonstrating the program’s impact on enhancing emergency response and patient care in the ICU.
Emergency Response Times and Interprofessional Collaboration
Utilization of NTCC service could potentially save up to 2.7 minutes per emergency response. The integration of simulation training has significantly increased the utilization of NTCC services, resulting in improved interprofessional collaboration, and enhanced speed and delivery of critical care interventions, ultimately leading to better patient outcomes:
- The average time for hospital providers to respond after emergency activation in the ICU nationally is 3.05 minutes (Arıkan et al., 2024; Morris et al., 2023; Patil et al., 2019; Weile et al., 2021; Winters et al., 2013).
- The average time for NTCC providers to respond after emergency activation in the ICU at NTCC affiliated facilities is 0.35 minutes (VA Telehealth, n.d.).
- The average time that could be saved using NTCC service per emergency response is 2.7 minutes.
Practice Barriers in Simulation
Excessive Autonomy
Excessive autonomy occurs when individual preferences lead to variability and complacency in practice standards (Veazie et al., 2019). This barrier can hinder the standardization and effectiveness of healthcare practices. To counteract excessive autonomy, the NTCC simulation incorporates several measures:
- Checklists: Standardized checklists ensure that all necessary steps are followed during critical care interventions, reducing variability, and enhancing consistency.
- Standardized emergency training: Regular training sessions provide opportunities for staff to practice and refine their skills in a controlled environment, reinforcing standardization and preparedness.
- Situation, Background, Assessment, Recommendation (SBAR): This standardized handoff tool ensures clear and concise communication between team members, reducing the risk of miscommunication and errors.
- Crew resource management models: These models promote team cohesion and effective collaboration, ensuring that all team members work together efficiently and effectively.
Craftsman Attitude
A craftsman attitude relies on specific individuals to carry out tasks, which can lead to dependency and variability in practice (Veazie et al., 2019). The NTCC simulation addresses this barrier by providing equivalent craftsmen resources and supporting shared mental models during crises. Key measures include:
- Rapid NTCC response: The NTCC team can respond to emergencies in 0.35 minutes on average, compared to the onsite emergency response team’s 3.05 minutes average response time (Veazie et al., 2019). This quick response ensures that critical care interventions are initiated promptly.
- Early cardiovascular resuscitation and role clarification: NTCC’s involvement ensures that resuscitation protocols are initiated early and that roles are clearly defined, enhancing the efficiency and effectiveness of the resuscitation efforts.
- Transition of emergency response team lead: The transition between NTCC and bedside teams is managed through quick debriefs, ensuring seamless coordination and continuity of care.
- Crowd control and triage assistance: NTCC team assists with crowd control and initial triage, ensuring that the resuscitation efforts are organized and efficient.
- Interprofessional collaboration: By bringing together experts from various specialties and disciplines, NTCC simulation ensures that all aspects of patient care are addressed comprehensively. This collaboration enhances the quality of care ensuring all team members contribute their unique perspectives and expertise.
Embracing HRO Principles
Deference to Practice
Deference to practice involves making decisions based on expertise rather than hierarchy (Veazie et al., 2019). Simulation training promotes this through:
- Assertive and respectful communication: The learners practice enhancing patient safety advocacy through clear and respectful communication, promoting team cohesion and inclusiveness.
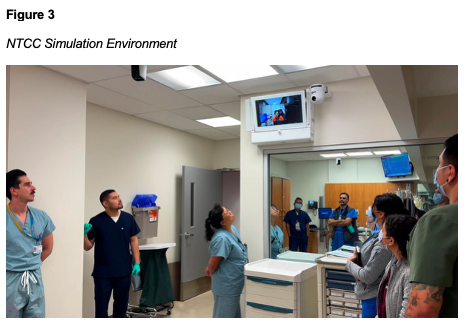
- Safe psychological environments: NTCC simulation creates safe environments for teams to practice and develop their skills, encouraging open communication and continuous improvement (Figure 3).
- Team lead training: Simulation provides education for novice team leaders, ensuring they are prepared to utilize all available resources effectively.
- Inclusive language: The use of inclusive language, such as “we,” “us,” and “let’s,” promotes a sense of teamwork and collaboration, reinforcing the idea that everyone is working together towards a common goal.
- Specific and direct communication: During simulations, communication is focused on being specific and direct, avoiding ambiguity and ensuring that instructions and feedback are clear and actionable.
Sensitivity to Operations
Sensitivity to operations emphasizes awareness of team dynamics and expertise (Veazie et al., 2019). During simulations, NTCC:
- Assists with crowd control and role confirmation: NTCC staff help confirm the roles and expectations of the emergency response team, ensuring that everyone knows their responsibilities and that the resuscitation efforts are coordinated and efficient.
- Promotes mutual expectations and shared mental models: By clarifying roles and expectations, NTCC ensures all team members are on the same page and can work together effectively.
- Encourages open dialogue and non-punitive communication: Creating an environment where team members feel comfortable speaking up and sharing their observations and suggestions are crucial for continuous improvement and patient safety.
- Increase situational awareness: By minimizing interruptions and distractions during emergencies, NTCC simulation enhances situational awareness to prevent and mitigate errors. This ensures that all team members are fully engaged and able to respond effectively in critical situations.
Conclusion
The NTCC Program, through its integration of advanced telehealth technologies and simulation training, exemplifies an innovative healthcare practice that enhances patient care outcomes and promotes a culture of safety. By aligning with HRO principles and leveraging interprofessional education through NTCC simulation, the speed and delivery of critical care interventions for Veterans improves. As the program continues to expand, its impact on Veteran care and healthcare simulation training will undoubtedly set new standards in critical care delivery.
References
Arıkan, M., Meriç, E., Yesilkaya, A., Tasdelen, B. N., & Akhan, A. (2024). Three-year retrospective analysis of code blue calls: single center experience. International Journal of Research in Medical Sciences, 12(5), 1471–1474. https://doi.org/10.18203/2320-6012.ijrms20241230
Morris, N. A., Couperus, C., Dezman, Z., Rubinson, L., Friedrich, R., Gurmu, S., & Lemkin, D. (2023). Feasibility of accelerated code team activation with code button triggered smartphone notification. Resuscitation, 187, 109752. https://doi.org/10.1016/j.resuscitation.2023.109752
Patil, V. C., Shah, J. N., Jedge, P. P., & Patil, S. V. (2019). Review of code blue system and audit. International Journal of Research in Medical Sciences, 7(5), 1809. https://doi.org/10.18203/2320-6012.ijrms20191681
Winters, B. D., Weaver, S. J., Pfoh, E. R., Yang, T., Pham, J. C., & Dy, S. M. (2013) Rapid-Response Systems as a Patient Safety Strategy: A Systematic review. Annals of Internal Medicine, 158(5), 417–425. https://doi.org/10.7326/0003-4819-158-5-201303051-00009
VA Telehealth. (n.d.). VA Telehealth Services. Retrieved June 4, 2024, from https://telehealth.va.gov/
Veazie, S., Peterson, K., & Bourne, D. (2019). Evidence Brief: Implementation of high reliability organization principles (VA ESP Project #09-199). Evidence Synthesis Program, Health Services Research and Development Service, Office of Research and Development, Department of Veterans Affairs. https://www.hsrd.research.va.gov/publications/esp/reports.cfm
Weile, J., Nebsbjerg, M. A., Ovesen, S. H., Paltved, C., & Ingeman, M. L. (2021). Simulation-based team training in time-critical clinical presentations in emergency medicine and critical care: a review of the literature. Advances in Simulation, 6(1). https://doi.org/10.1186/s41077-021-00154-4