Authors
Isra K. Elsaadany, BS1, Hang-Ling Wu, BS2, Jessica M. Gonzalez-Vargas, PhD3, Jason Z. Moore, PhD2, Scarlett R. Miller, PhD1,3
1Department of Industrial and Manufacturing Engineering, Penn State, University Park, PA
2Department of Mechanical and Nuclear Engineering, Penn State, University Park, PA
3School of Engineering Design and Innovation, Penn State, University Park, PA
Conflict of Interest Statement
Research reported in this work was supported by Chester Ray Trout Chair in Pediatric Surgery at Penn State’s Children Hospital. The content is solely the responsibility of the authors and does not necessarily represent the official views of Chester Ray Trout Chair in Pediatric Surgery at Penn State’s Children Hospital. Coauthor Dr. Miller and Dr. Moore owns equity in Medulate, which may have a future interest in this project. Company ownership has been reviewed by the University’s Individual Conflict of Interest Committee and is currently being managed by the University.
Corresponding Author
Scarlett R. Miller, PhD, Department of Industrial and Manufacturing Engineering, School of Engineering Design and Innovation, Penn State, University Park, PA
(Email: scarlettmiller@psu.edu)
Abstract
Introduction: In recent years, pediatric minimally invasive surgery (MIS) has grown, which is more complex than adult MIS. Serious complications can occur, but raining can decrease these risks. While medical simulation-based training (SBT) is effective, pediatric SBT is still in its infancy. Pediatric laparoscopic surgery (PLS) is one form of MIS that requires effective training. Thus, the goal of our study was to design an Augmented Reality (AR) and a pediatric simulator, then assess the impact of SBT with and without AR on PLS self-efficacy and performance.
Methods: Twelve novice residents and fourteen medical students from Hershey Medical Center were assigned to one training condition and completed a peg transfer task, with or without AR feedback, and starting with a regular box trainer (BT) (easier) first, then on the pediatric trainer (PT) (harder), or vice versa. Self-efficacy in laparoscopic surgery and practices was assessed using an 18-item questionnaire on a 5-point Likert scale. Time and number of pegs dropped were measured during the task.
Results: Wilcoxon signed rank tests revealed that self-efficacy improved pre- to post-training on the 18 self-efficacy statements (p < 0.05). Two-way ANOVA showed that starting with the easier BT first then on the PT improved time performance in the PT (p = 0.003). Hoteling’s T2 revealed no significant difference in performance with AR feedback (p > 0.05).
Conclusions: SBT with and without AR can improve self-efficacy in PLS and starting with either task may improve performance in more complex tasks. Future work will develop and evaluate the effectiveness of AR feedback.
Introduction
Minimally Invasive Surgery (MIS) is performed by surgeons to operate on patients using small incisions, to minimize damage to the patient’s body compared to open surgery (Anand et al., 2022) and to allow a quicker recovery, reduced pain, and shorter hospitalization duration (Dagorno et al., 2021). Specifically, pediatric MIS on children has increased rapidly over the last decade. However, there are technical challenges due to the diverse sizes and physiological differences within the pediatric population (Pogorelić, 2022). Due to the greater technical complexity of pediatric surgery compared to general surgery, caution and safety are essential during the procedure (Yokoyama et al., 2019). Additionally, pediatric MIS necessitates more psychomotor effort and skill from surgeons to account for smaller instruments and motion scaling compared to regular laparoscopic surgery (Hamilton et al., 2011).
Patient outcomes can also be impacted due to the learning curve associated with pediatric MIS (Uecker et al., 2020). Research has also shown that complication rates in pediatric MIS can reach up to 17% which includes bowel obstruction, bile leakage and infections (Uecker at al., 2020). The risks of these complications can decrease with experience and learning skills (Sa et al., 2016), and training and education (Esposito et al., 2019). However, pediatric simulation-based training (SBT) is still in its ‘infancy’ (Skertich et al., 2020). As such, more research in pediatric SBT is required. In addition, laparoscopic surgery is one form of MIS that requires more effective teaching strategies (Gallagher et al., 2003).
SBT has been shown to be effective in improving performance and reducing complications in medical training (Aydin et al., 2021). Specifically, self-efficacy, which is a measure of a trainee’s confidence in carrying out a procedure or in providing patient care based on their own self-evaluation, is an important construct in SBT (Themason & Rosen, 2014). It has been linked to enhanced performance (Themason & Rosen, 2014) and is a critical component of safe surgical techniques and understanding of one’s own capabilities (Anderson et al., 2020). However, approximately 92.3% of residents express shortcomings in their ability to perform medical procedures independently (Anderson et al., 2020). As such, Augmented Reality (AR) simulators are one form of SBT that can improve patient safety (Barsom et al., 2016), performance in surgeries (Williams et al., 2020) and confidence (Chiang et al., 2021). In addition, research indicates that simulation order with regards to starting with easier simulation training before advancing to more complex simulations, enhances performance during SBT (Brydges et al., 2010). Therefore, the goal of this study was to develop a new AR and pediatric simulator for laparoscopic training and understand the impact of SBT with and without AR on self-efficacy and performance in pediatric laparoscopic surgery (PLS).
Methods
This study aims to answer the following research questions (RQ).
RQ1: Do novices improve their pediatric laparoscopic self-efficacy over the course of simulation training?
The goal of this RQ was to understand whether novice’s self-efficacy in PLS improves from pre- to post-simulation training. We hypothesize that laparoscopic self-efficacy will improve after training because prior work has shown that SBT can improve confidence in laparoscopic surgery (Barnes et al., 2015).
RQ2: Does simulation task order impact pediatric laparoscopic performance?
The goal of this RQ was to understand whether simulation order, starting with an easier task (regular box trainer) and then finishing with a harder task (pediatric trainer) or vice versa, would affect trainees’ performance. It was hypothesized that performance in the harder task (pediatric) would improve when performed first on the easier task (regular) since research has shown that increasing the level of difficulty during simulation training improves performance (Brydges et al., 2010).
RQ3: Does providing AR feedback during simulation training improve performance?
The goal of this RQ was to understand whether providing visual AR feedback improves performance during laparoscopic training. It was hypothesized that individuals who received visual feedback during the task will perform better because prior work has shown that visual feedback during laparoscopic training can improve performance (Horeman et al., 2014).
Participants
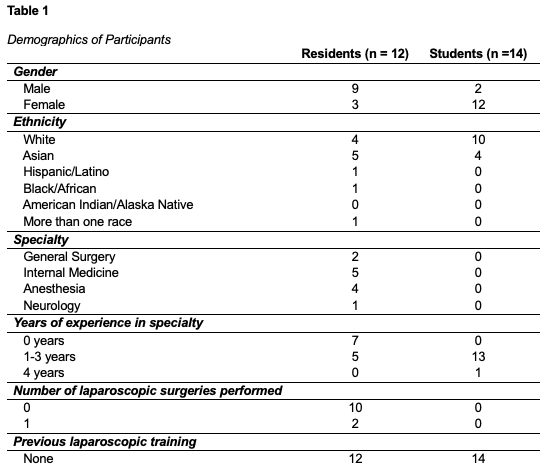
A total of 26 participants were recruited over two sessions from Hershey Medical Center. The first session included 11 medical residents. While the second session included 14 medical students and 1 resident. All participants were novices since they either performed less than 50 laparoscopic procedures or had no prior experience with the procedure (Buznik et al., 2008). Demographics of the participants are reported in Table 1.
Study Equipment
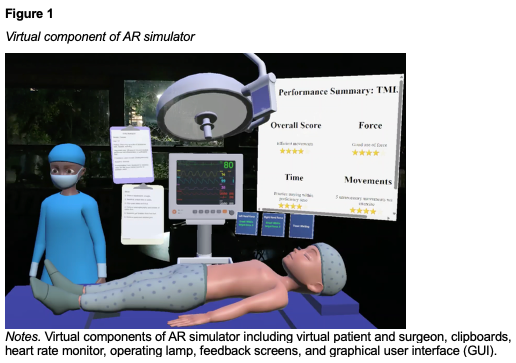
An AR simulator was created using the Microsoft HoloLens 2, Unity software (version 2021.3.6), and the Mixed Reality Toolkit (version 1.2209.0). Specifically, this simulator was developed to provide more realistic training conditions and visualizations, haptic feedback and real-time feedback on force and time, see Figure 1. Feedback included digits turning red when the proficiency time exceeded the 48-seconds FLS standard (SAGES FLS committee, 2019) or force exceeded 0.4N (based on sensitivity of sensors). The AR simulator also includes a virtual patient, surgeon, and clipboard with training instructions.
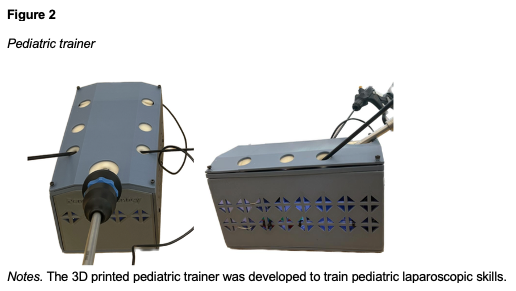
A 3D-printed pediatric trainer was developed which allows training of fundamental laparoscopic surgery (FLS) skills (SAGES FLS committee, 2019), see in Figure 2. We used the baseball diamond principle (Ismail & Mishra, 2014) to triangulate the instruments, resulting in the first port insertion for the laparoscopic camera, and the other two ports for the laparoscopic graspers, see Figure 2. This principle was also used to determine the dimensions of the pediatric trainer, resulting in measurements of 140 mm x 230 mm x 126 mm (Ismail & Mishra, 2014). The trainer also included a suture pad which is used as the abdominal ports for instrument insertion. A commercially available standard ‘box trainer’ for laparoscopic training was also used in this study with dimensions 455 mm x 395 mm x 220 mm. The Tobii Pro 3 eye trackers were also utilized to track eye gaze data.
Procedure
First, procedures were explained and informed consent was obtained. Participants were compensated with $15 and completed four surveys: prior FLS experience, pre-self-efficacy, NASA Task Load Index (NASA-TLX) and mental workload. Next, Next, they were assigned to their condition. Participants in the first session were assigned to start with the Box Trainer (BT – easier) first: (1) Box Trainerno feedback then on Pediatric trainerno feedback, (2) Box trainerno feedback then on Pediatric Trainerfeedback, (3) Box trainerfeedback then Pediatric trainernofeedback, or (4) Box Trainerfeedback then Pediatric Trainerfeedback.
Participants in the second session were assigned to the same conditions but starting with the Pediatric Trainer (PT – harder) first: (1) Pediatric Trainerno feedback then on Box Trainerno feedback, (2) Pediatric Trainerno feedback then on Box Trainerfeedback, (3) Pediatric Trainerfeedback then Box Trainernofeedback, or (4) Pediatric Trainerfeedback then Box Trainerfeedback. In the feedback conditions, participants used the HoloLens over eye trackers and watched a 32-instructional video about the AR simulator. This fundamental skill required residents to use the laparoscopic graspers to grab each of the 6 colored pegs from the pegboard with their non-dominant hand, transfer it mid-air to their dominant hand, and place it on the opposite side of the pegboard. After each task in each condition, participants completed 4 surveys: post-self-efficacy, NASA-TLX, workload and validation questionnaires.
Outcome Measures
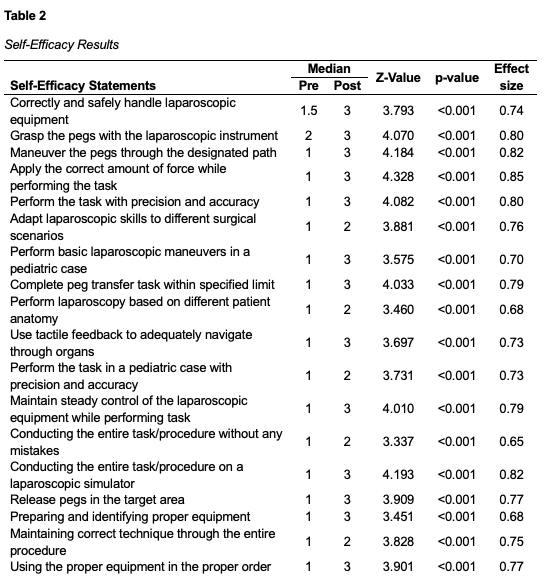
The main outcomes were self-efficacy, simulation order, time, and number of errors. Self-efficacy was assessed with 18-item Likert Scale from “Not at all confident” (1) to “Extremely confident” (5), see Table 2. Simulation order was based on whether participants started with the BT or PT first. Time was recorded from picking up the first peg to releasing the sixth (SAGES FLS Committee, 2019). Number of errors was quantified by the number of dropped pegs (Rhee et al., 2014).
Statistical Analysis
All statistics were analyzed with SPSS (version 29.0) with a significance level 0.05. A Wilcoxon Signed-Rank Test determined statistical significance between the pre- and post-surveys (independent variables) on each of the 18 self-efficacy statement scores (dependent variable). The difference scores were approximately symmetrically distributed, as assessed by a histogram with superimposed normal curve. Data are expressed as median values.
Two Two-Way Mixed ANOVAs were conducted to examine the effects of simulation order (between-subjects factor) and type of trainer (box trainer vs pediatric trainer, within-subjects factor) on two dependent variables: time and number of errors. Assumption checks indicated that the data met the requirements for ANOVA. The dependent variables were normally distributed, as assessed by Shaprio-Wilk’s test (p > 0.05), and there was homogeneity of variances (Levene’s test, p > 0.05) and homogeneity of covariances (Box’s M test, p = 0.113). However, Mauchly’s test indicated a violation of sphericity for the two-way interaction (p < 0.05).
Lastly, a Hoteling’s T2 examined whether providing feedback through AR (independent variable) impacts time and number of errors (dependent variables). For both trainer types, the data were normally distributed (Shapiro-Wilk test, p > 0.05), and no univariate or multivariate outliers were identified based on boxplots and Mahalanobis distance (p > 0.001), respectively. Relationships between variables were linear as assessed by scatterplots, and no multicollinearity was detected (|r| < 0.9). Homogeneity of variance-covariance matrices was confirmed (Box’s M test, p = 0.205). Data are expressed as mean ± standard deviation.
Results
RQ1: Do novices improve their pediatric laparoscopic self-efficacy over the course of simulation training?
A Wilcoxon-signed rank test showed a statistically significant median increase in pediatric laparoscopic post-self-efficacy compared to the pre-self-efficacy for all 18 statements (p < 0.05), with strong effect sizes of greater than 0.70, see Table 2.
RQ2: Does simulation task order impact pediatric laparoscopic performance?
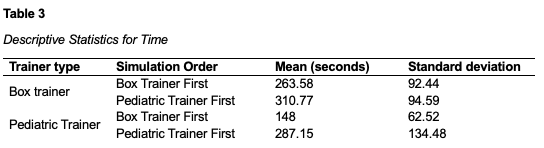
A two-way Mixed ANOVA was performed to evaluate the effects of simulation order and type of trainer on task completion time. The means and standard deviations for completion time are presented in table 3 below. Data are reported as mean ± standard deviation (SD). The results indicated a significant interaction effect between simulation order and type of trainer on time, F(1,23) = 5.278, p = 0.025, partial η2 = 0.199. Simple main effects indicated that time was not statistically significant different between starting with easier box first than starting with pediatric first on the box trainer (p = 0.220). Simple main effects indicated that time was significantly lower when starting with easier box trainer first than starting with pediatric trainer first on the pediatric trainer (p=0.003).
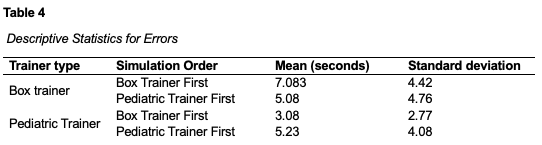
Another two-way mixed ANOVA indicated a significant interaction effect between simulation order and type of trainer on number of errors, F(1,23) = 5.120, p = 0.033, partial η2 = 0.182. The means and standard deviations for number of errors are presented in table 4 below. Simple main effects indicated that number of errors was not statistically significant different between starting with easier box first than starting with pediatric first on the box trainer (p = 0.288). Simple main effects showed that number of errors was significant lower on pediatric trainer than box trainer in easier box trainer first, F(1,11) = 7.040, p = 0.022, partial η2 = 0.390. Simple main effects showed that number of errors was not significant on any type of trainer in pediatric trainer first F(1,12) = 0.02, p = 0.890, partial η2 = 0.002.
RQ3: Does providing AR feedback during simulation training improve performance?
In the BT simulation task, participants without AR feedback demonstrated shorter task times (281.4 ± 100) and fewer errors (5 ± 4.4) compared to the task times (295.4 ± 92.4) and errors (7.2 ± 4.7) in the AR feedback. However, these differences were not statistically significant, F(2,22) = 0.667, p = 0.523, Wilks’ Λ = 0.943, partial η2 = 0.057. Similarly, on the PT, participants without AR feedback showed shorter task times (211.8 ± 83.67) and fewer errors (3.6 ± 2.7) compared to the task times (233.3 ± 164.6) and errors (5.2 ± 4.2) in the AR feedback. Moreover, these differences were not statistically significant, F(2,21) = 0.679, p = 0.518, Wilks’ Λ = 0.939, partial η2 = 0.061.
Discussion
The goal of this study was to understand the impact of SBT with and without AR on PLS performance. For the first RQ, we found that novices self-efficacy improved from pre to post training in PLS, supporting our hypothesis that simulation-based training improves self-efficacy. Specifically, pediatric SBT with and without AR improved novices’ self-efficacy. High self-efficacy is scientifically associated with effective application of acquired skills (Smith et al., 1995), and sufficient confidence is necessary for safe clinical practice (Gottlieb et al., 2021).
For the second RQ, we found that starting with an easier simulation task (BT) then progressing to a more complex task (PT), improved time performance in the PT task, but not for number of errors, partially supporting our hypothesis. This holds importance in medical simulation training because starting from easier to more difficult tasks during simulation training improves performance in the operating room (Grover et al., 2017). For our third RQ, we found that providing AR visual feedback during simulation training did not improve performance, refuting our hypothesis. This aligns with prior research showing no differences in performance with AR feedback, and participants also took longer to complete the task with feedback (Zahiri et al., 2017). Attentional selectivity, the ability to focus on task-relevant stimuli and ignore distractions can be a sign of expertise (Stefanidis et al., 2007). In addition, skilled surgeons can maintain selective intention and block out distractions (Anton et al., 2018), a quality our novice participants may have lacked, which could have affected their utilization of the AR feedback during the tasks.
Limitations in this study include a small sample size and variability of participants. In addition, due to time constraints of medical residents and students, they were only asked to complete half of the peg transfer task. Future work will analyze eye gaze data of novices and compare it with experts, to further understand the effectiveness of AR feedback during simulation-training. This could potentially help us identify strategies to train and increase novices’ attentiveness to task relevant stimuli during their training to improve their performance. Future work will improve the fidelity of the AR simulator and ensure participants complete the full task.
Conclusion
To improve PLS training, an AR simulator with a pediatric laparoscopic trainer was developed, and the study aimed to determine the impact of SBT with and without AR in this field. The results of our study showed that pediatric laparoscopic self-efficacy of novices improved with and without AR training, simulation task order improved time performance in the harder pediatric task and providing AR visual feedback did not impact performance. This highlights the potential benefits of simulation training in improving self-efficacy and performance in PLS; however, more work is required to determine the full effectiveness of AR during training. As such, SBT with and without AR may work towards improving skill acquisition in PLS.
References
Anand, S., Pogorelić, Z., Singh, A., Muñoz, C. L., Krishnan, N., Dhua, A., Goel, P., & Bajpai, M. (2022). Comparison of Unnoticed Glove Perforations during Minimally Invasive versus Open Surgeries: A Systematic Review and Meta-Analysis. Children, 9(2), 179. https://doi.org/10.3390/children9020179
Anderson, T. N., Payne, D. H., Dent, D. L., Kearse, L. E., Schmiederer, I. S., & Korndorffer, J. R. (2020). Defining the deficit in US surgical Training: The Trainee’s perspective. Journal of the American College of Surgeons, 232(4), 623–627. https://doi.org/10.1016/j.jamcollsurg.2020.11.029
Anton, N. E., Mizota, T., Timsina, L. R., Whiteside, J. A., Myers, E. M., & Stefanidis, D. (2018). Attentional selectivity, automaticity, and self-efficacy predict simulator-acquired skill transfer to the clinical environment. The American Journal of Surgery, 217(2), 266–271. https://doi.org/10.1016/j.amjsurg.2018.11.028
Aydın, A., Ahmed, K., Abe, T., Raison, N., Van Hemelrijck, M., Garmo, H., Ahmed, H. U., Mukhtar, F., Al-Jabir, A., Brunckhorst, O., Shinohara, N., Zhu, W., Zeng, G., Sfakianos, J. P., Gupta, M., Tewari, A., Gözen, A. S., Rassweiler, J., Skolarikos, A., . . . Dasgupta, P. (2021). Effect of simulation-based training on surgical proficiency and patient outcomes: a randomised controlled clinical and educational trial. European Urology, 81(4), 385–393. https://doi.org/10.1016/j.eururo.2021.10.030
Barnes, J., Burns, J., Nesbitt, C., Hawkins, H., & Horgan, A. (2015). Home virtual reality simulation training: the effect on trainee ability and confidence with laparoscopic surgery. Journal of Surgical Simulation, 2. https://doi.org/10.1102/2051-7726.2015.0012
Barsom, E. Z., Graafland, M., & Schijven, M. P. (2016). Systematic review on the effectiveness of augmented reality applications in medical training. Surgical Endoscopy, 30(10), 4174–4183. https://doi.org/10.1007/s00464-016-4800-6
Brydges, R., Carnahan, H., Rose, D., Rose, L., & Dubrowski, A. (2010). Coordinating progressive levels of simulation fidelity to maximize educational benefit. Academic Medicine, 85(5), 806–812. https://doi.org/10.1097/acm.0b013e3181d7aabd
Buzink, S. N., Botden, S. M. B. I., Heemskerk, J., Goossens, R. H. M., De Ridder, H., & Jakimowicz, J. J. (2008). Camera navigation and tissue manipulation; are these laparoscopic skills related? Surgical Endoscopy, 23(4), 750–757. https://doi.org/10.1007/s00464-008-0057-z
Chiang, F., Shang, X., & Qiao, L. (2021). Augmented reality in vocational training: A systematic review of research and applications. Computers in Human Behavior, 129, 107125. https://doi.org/10.1016/j.chb.2021.107125
Dagorno, C., Montalva, L., Ali, L., Brustia, R., Paye-Jaquen, A., Pio, L., & Bonnard, A. (2021). Enhancing recovery after minimally invasive surgery in children: A systematic review of the literature and meta-analysis. Journal of Pediatric Surgery, 56(12), 2157–2164. https://doi.org/10.1016/j.jpedsurg.2021.04.004
Esposito, C., Becmeur, F., Steyaert, H., & Szavay, P. (2019). ESPES Manual of Pediatric Minimally Invasive Surgery. In Springer eBooks. https://doi.org/10.1007/978-3-030-00964-9
Gallagher, A. G., Ritter, E. M., & Satava, R. M. (2003). Fundamental principles of validation, and reliability: rigorous science for the assessment of surgical education and training. Surgical Endoscopy, 17(10), 1525–1529. https://doi.org/10.1007/s00464-003-0035-4
Gottlieb, M., Chan, T. M., Zaver, F., & Ellaway, R. (2021). Confidence‐competence alignment and the role of self‐confidence in medical education: A conceptual review. Medical Education, 56(1), 37–47. https://doi.org/10.1111/medu.14592
Grover, S. C., Scaffidi, M. A., Khan, R., Garg, A., Al-Mazroui, A., Alomani, T., Yu, J. J., Plener, I. S., Al-Awamy, M., Yong, E. L., Cino, M., Ravindran, N. C., Zasowski, M., Grantcharov, T. P., & Walsh, C. M. (2017). Progressive learning in endoscopy simulation training improves clinical performance: a blinded randomized trial. Gastrointestinal Endoscopy, 86(5), 881–889. https://doi.org/10.1016/j.gie.2017.03.1529
Hamilton, J. M., Kahol, K., Vankipuram, M., Ashby, A., Notrica, D. M., & Ferrara, J. J. (2011). Toward effective pediatric minimally invasive surgical simulation. Journal of Pediatric Surgery, 46(1), 138–144. https://doi.org/10.1016/j.jpedsurg.2010.09.078
Horeman, T., Van Delft, F., Blikkendaal, M. D., Dankelman, J., Van Den Dobbelsteen, J. J., & Jansen, F. (2014). Learning from visual force feedback in box trainers: tissue manipulation in laparoscopic surgery. Surgical Endoscopy, 28(6), 1961–1970. https://doi.org/10.1007/s00464-014-3425-x
Ismail, A. J., & Mishra, R. (2014). Comparing Task Performance and Comfort during Nonpulmonary Video-assisted Thoracic Surgery Procedures between the Application of the ‘Baseball Diamond’ and the ‘Triangle Target’ Principles of Port Placement in Swine Models. World Journal of Laparoscopic Surgery With DVD, 7, 60–65. https://doi.org/10.5005/jp-journals-10033-1218
Pogorelić, Z. (2022). Advances and future challenges of minimally invasive surgery in children. Children, 9(12), 1959. https://doi.org/10.3390/children9121959
Rhee, R., Fernandez, G., Bush, R., & Seymour, N. E. (2014). The effects of viewing axis on laparoscopic performance: a comparison of non-expert and expert laparoscopic surgeons. Surgical Endoscopy, 28(9), 2634–2640. https://doi.org/10.1007/s00464-014-3515-9
Sa, W., Gn, M., Na, B., Aa, B., S, K., & Fh, A. (2016). Our experience of laparoscopic surgery in children during the learning curve. Medical Reports & Case Studies, 01(01). https://doi.org/10.4172/2572-5130.1000102
SAGES FLS committee. (2019). Technical Skills Proficiency-Based Training Curriculum. In Fundamentals of Laparoscopic Surgery. https://www.flsprogram.org/wp-content/uploads/2014/02/Proficiency-Based-Curriculum-updated-May-2019-v24-.pdf
Skertich, N. J., Schimpke, S. W., Lee, T., Wiegmann, A. L., Pillai, S., Rossini, C., Madonna, M. B., & Shah, A. N. (2020). Pediatric Surgery Simulation-Based Training for the General Surgery Resident. Journal of Surgical Research, 258, 339–344. https://doi.org/10.1016/j.jss.2020.05.038
Smith, R. C., Mettler, J. A., Stöffelmayr, B. E., Lyles, J. S., Marshall, A. A., Van Egeren, L. F., Osborn, G. G., & Shebroe, V. (1995). Improving residents’ confidence in using psychosocial skills. Journal of General Internal Medicine, 10(6), 315–320. https://doi.org/10.1007/bf02599950
Stefanidis, D., Scerbo, M. W., Korndorffer, J. R., & Scott, D. J. (2007). Redefining simulator proficiency using automaticity theory. The American Journal of Surgery, 193(4), 502–506. https://doi.org/10.1016/j.amjsurg.2006.11.010
Themanson, J. R., & Rosen, P. J. (2014). Examining the relationships between self‐efficacy, task‐relevant attentional control , and task performance: Evidence from event‐related brain potentials. British Journal of Psychology, 106(2), 253–271. https://doi.org/10.1111/bjop.12091
Uecker, M., Kuebler, J. F., Ure, B. M., & Schukfeh, N. (2020). Minimally Invasive Pediatric Surgery: the learning curve. European Journal of Pediatric Surgery, 30(02), 172–180. https://doi.org/10.1055/s-0040-1703011
Williams, M. A., McVeigh, J., Handa, A. I., & Lee, R. (2020). Augmented reality in surgical training: a systematic review. Postgraduate Medical Journal, 96(1139), 537–542. https://doi.org/10.1136/postgradmedj-2020-137600
Yokoyama, S., Mizunuma, K., Kurashima, Y., Watanabe, Y., Mizota, T., Poudel, S., Kikuchi, T., Kawai, F., Shichinohe, T., & Hirano, S. (2019). Evaluation methods and impact of simulation-based training in pediatric surgery: a systematic review. Pediatric Surgery International, 35(10), 1085–1094. https://doi.org/10.1007/s00383-019-04539-5
Zahiri, M., Nelson, C. A., Oleynikov, D., & Siu, K. (2017). Evaluation of augmented reality feedback in surgical training environment. Surgical Innovation, 25(1), 81–87. https://doi.org/10.1177/1553350617739425