Authors
Peter L. Stallo, PhD1, Suzan Kardong-Egren, PhD1, Eric B. Bauman, PhD1
1Massachusetts General Hospital Institute of Health Professions, Department of Health Professions Education, Boston, MA
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Corresponding Author
Peter L. Stallo, CRNA, PhD, Massachusetts General Hospital Institute of Health Professions,
Department of Health Professions Education, Boston, MA
Abstract
Background: Although a wide range of factors have been implicated in the development of cybersickness, the target headset selection has also been identified as a significant contributing factor. This study compares measures of cybersickness between the Meta Quest 2 and Meta Quest Pro headsets.
Methods: Thirty-four subjects between the ages of 19 and 30 participated in a threeminute-long simulated roller-coaster ride. Differences in Simulation Sickness Questionnaire (SSQ) scores and measurements taken from a hand-held dial that allowed for the moment-tomoment recording of discomfort levels were recorded.
Results: Significant findings include decreased SSQ scores for participants using the Meta Quest Pro headset and increases in the oculomotor and disorientation components of the SSQ score related to interpupillary distance (IPD) mismatch.
Conclusion: As researchers consider the implementation of VR headsets for a particular application, it would be prudent to evaluate the IPD adjustability of the headset in question. By comparing it to the typical IPD range of the population where it will be deployed, it may be possible to reduce the contribution of IPD mismatch on the severity and incidence of cybersickness.
Introduction
Virtual Reality (VR) training offers an opportunity to increase engagement in students by encouraging active participation through physical interaction with objects in the virtual environment (Fabris, et al., 2019) and allowing for a greater understanding of concepts through self-directed inquiry and exploration (Maresky et al., 2019). However, cybersickness, a form of motion sickness experienced within Head-Mounted Device (HMD) virtual reality devices, poses a threat to the quality of the VR educational experience. Occurring in as many as 40% of participants (Moro et al., 2017), cybersickness impedes the deployment of VR within institutional settings.
The technical capabilities of HMDs differ substantially, and these differences have been shown to be contributing factors in the development of cybersickness (Caserman et al., 2021).
As universities contemplate investments in VR, price is a significant consideration. For example, the Meta Quest 2 was priced at $399 on release compared to $1499 for the Meta Quest Pro (Meta Quest Pro Vs Meta Quest 3 (Comparison) - VRcompare, 2023). However, if the technological advancements in newer, more expensive headsets contribute to a significant decrease in cybersickness symptoms, the additional investment may increase the effectiveness of VR learning experiences. Currently, there are no published studies evaluating these two headsets for any differences in their associated incidence and severity of cybersickness. For this reason, understanding the degree to which more advanced HMDs may mitigate cybersickness is crucial in maximizing the effectiveness of VR and promoting its adoption as an experiential medium.
Motion Sickness Nomenclature
The term ‘cybersickness’ was first coined by McCauley and Sharkey (1992) to refer to motion sickness symptoms that specifically occur in HMD virtual reality. While the terms ‘cybersickness’ and ‘VR sickness’ are synonyms describing identical symptomatology (Chang et al., 2020; Gallagher & Ferre, 2018; Saredakis et al., 2020), they are distinct from other terms seen in the literature such as motion sickness, simulation sickness, and visually induced motion sickness. Motion sickness encompasses all symptoms that result from motion, whether it is real or simulated. Simulation sickness refers to motion sickness symptoms that occur during a simulated experience whether it be virtual reality, fixed-base aircraft simulators, or driving simulators (Kennedy et al., 1993). Visually induced motion sickness is a subset of simulator sickness resulting from the use of visual display devices to simulate an experience. This includes VR, immersive rooms, cinemas, and video game systems (Keshavarz et al., 2019).
HMD Selection and Cybersickness
Gender (Stanney et al., 2020), age (Arns & Cerney, 2005), anxiety level (Paillard et al., 2013), manner of locomotion (Kim & Rhiu, 2021; Lin et al., 2022; Mayor et al., 2021) , and manner of presentation of visual information (Budhiraja et al., 2017; Liu & Chen, 2022; Won & Kim, 2022) have all been identified as factors in the development of cybersickness. Additionally, the target headset selection has been identified as a significant contributing factor (Caserman et al., 2021).
VR headsets vary significantly in their technical specifications (Table 1). For example, when comparing the Meta Quest 2 and the Meta Quest Pro, the Meta Quest Pro headset contains a faster processor and a faster default refresh rate of 120 Hz compared to 90 Hz in the Meta Quest 2, which could result in less latency (Heaney et al., 2023). Increased latency can result in display lag, a situation where the movements of the user’s view in the virtual world are delayed significantly enough from the real-world movement of their head to produce cybersickness (Kim, Luu, & Palmisano, 2022).
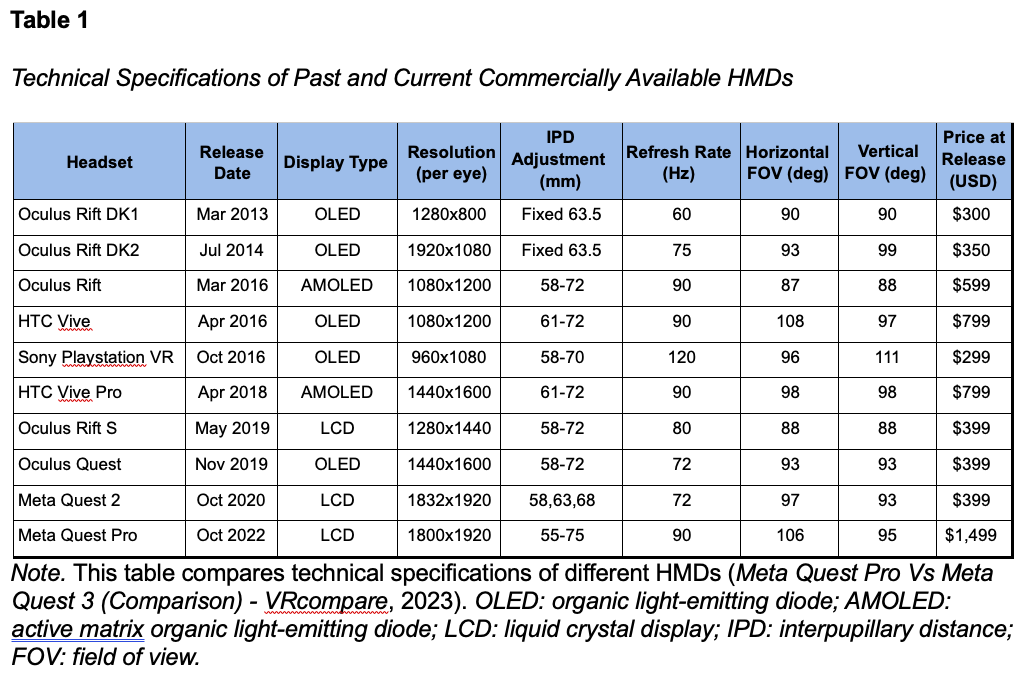
Headsets also differ in their ability to adjust the interpupillary distance (IPD), which has been shown to be the primary driver of gender-based differences in motion sickness (Stanney et al., 2020). The Meta Quest 2 has only three possible IPD settings: 58, 63, and 68 mm. In contrast, the Meta Quest Pro is continuously adjustable between 55 and 75 mm.
Measuring Cybersickness and Predisposition to Cybersickness
For the purposes of this research, the Simulator Sickness Questionnaire (SSQ) (Kennedy, 1993) was used to assess perceived simulation symptoms before and after the intervention. The Motion Sickness Susceptibility Questionnaire (MSSQ) short form (Golding, 1998) and the Visually Induced Motion Sickness Susceptibility Questionnaire (VIMSSQ) short form, also developed by Golding (2021), were used to assess predisposition to motion sickness symptoms.
The SSQ elicits responses for 16 different symptoms categorized as components of nausea, oculomotor symptoms, or disorientation (Kennedy, 1993). Total SSQ scores range from 0 to 235 (Walter et al, 2019). Based on data obtained from studies on military pilots, SSQ scores are categorized as follows: less than 5 is negligible, 5-10 is minimal, 11-15 is significant, and 16-20 is concerning (Bimberg, 2020).
The MSSQ evaluates the childhood and adult history of motion sickness on various modes of transportation. The raw MSSQ scores range from 0, indicating never experiencing any of the modes, to 54, indicating frequently feeling sick on all modes. The scoring for each mode is as follows: 0 is never felt sick, 1 is rarely felt sick, 2 is sometimes felt sick, and 3 is frequently felt sick.
The VIMSSQ assesses susceptibility to five different symptoms: headache, fatigue, dizziness, nausea, and eyestrain. These symptoms can occur when using visual display devices such as smartphones, tablets, video games, and virtual reality glasses. The score ranges from 0, which indicates no symptoms, to a maximum of 18. Higher scores indicate greater susceptibility to visually induced motion sickness symptoms
Eliciting Cybersickness
Because of the significant disparity in virtual versus real-world motion, the standard experience for eliciting cybersickness in virtual reality is a simulated roller coaster ride (Eftekharifar et al., 2021; Gavgani et al., 2017; Grassini et al., 2021; Nesbitt et al., 2017; Stanney et al., 2020). For this study, we used the commercially available Epic Roller Coaster software by B4T Games (Balneário Camboriú, Brazil). The roller-coaster simulation consisted of a three-minute first-person view in the seated position.
Methods
Participants
After receiving IRB approval, thirty-four subjects, 15 males and 19 females, were recruited from a university nursing program to participate in the study. Participants were between the ages of 20 and 34. Inclusion criteria include the following: willingness to participate, binocular vision with or without corrective lenses, and no restriction that would prevent the donning of a virtual reality headset. Exclusion criteria include the following: known history of significant motion sickness, known history of motion sickness lasting longer than 15 minutes produced by virtual reality use, known severe history of balance disorder or dizziness, known history of seizure disorder, known cardiac condition, known migraine disorder, current cold or flu symptoms, alcohol use within the past 12 hours, pregnancy at the time of data collection, known history of severe hearing deficit, and age less than 18 years. An explanation of the testing procedure was provided before obtaining signed consent to participate.
Study Procedure
Prior to beginning the roller-coaster simulation, participants completed the Motion Sickness Susceptibility Questionnaire (MSSQ), the Visually Induced Motion Sickness
Susceptibility Questionnaire (VIMSSQ) short form, and a baseline Simulator Sickness Questionnaire (SSQ) questionnaire. In addition, a brief demographic questionnaire was obtained.
During the roller-coaster simulation, subjects used a handheld device, called the discomfort dial, with a roller wheel to indicate their current level of motion sickness severity. The discomfort levels ranged from 0 to 10. Subjects were informed that discomfort levels were categorized as follows: level 1 is no discomfort, levels 2-4 are mild discomfort, levels 4-7 are moderate discomfort, and levels 8-10 are severe discomfort. The device provided audio feedback indicating the numeric level of severity to a wireless speaker mounted near the subject.
Participants were then randomly assigned to either the Meta Quest 2 or Meta Quest Pro group. Participant demographics are presented in Table 2. The Meta Quest 2 group consisted of 9 males and 8 females with an average age of 24.2 ± 3.7 years. The Meta Quest Pro group consisted of 6 males and 11 females with an average age of 24.8 ± 3.9 years.
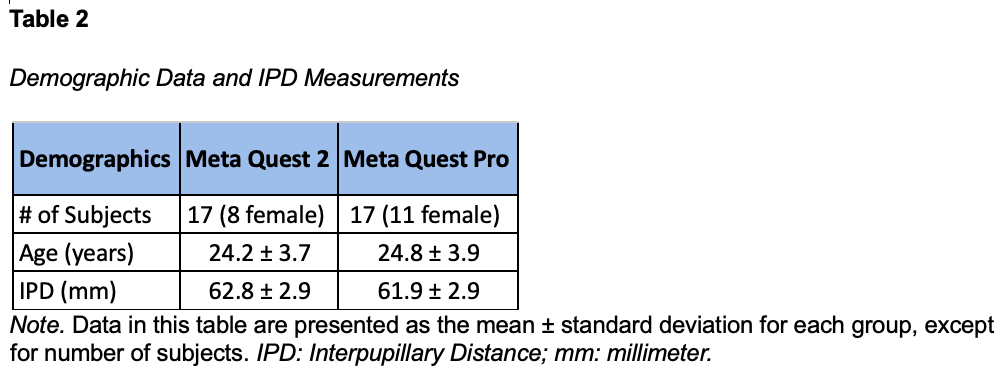
The participants' interpupillary distances were measured and averaged for each group (Table 2). The Meta Quest 2 group exhibited an average IPD of 62.8 ± 2.9 millimeters. The Meta Quest Pro group exhibited an average IPD of 61.9 ± 2.9 millimeters. The IPD setting of the device was adjusted to match the participant. If a participant did not match one of the three IPD settings on the Meta Quest 2 headset, then the nearest IPD was used. If the participant’s IPD was exactly in between two of the three available Meta Quest 2 IPD settings, then the higher IPD setting was used. No individuals exhibited an IPD measurement outside of the minimum and maximum IPD range of either device. Immediately following the roller-coaster simulation, each participant completed the SSQ again.
Data Analysis
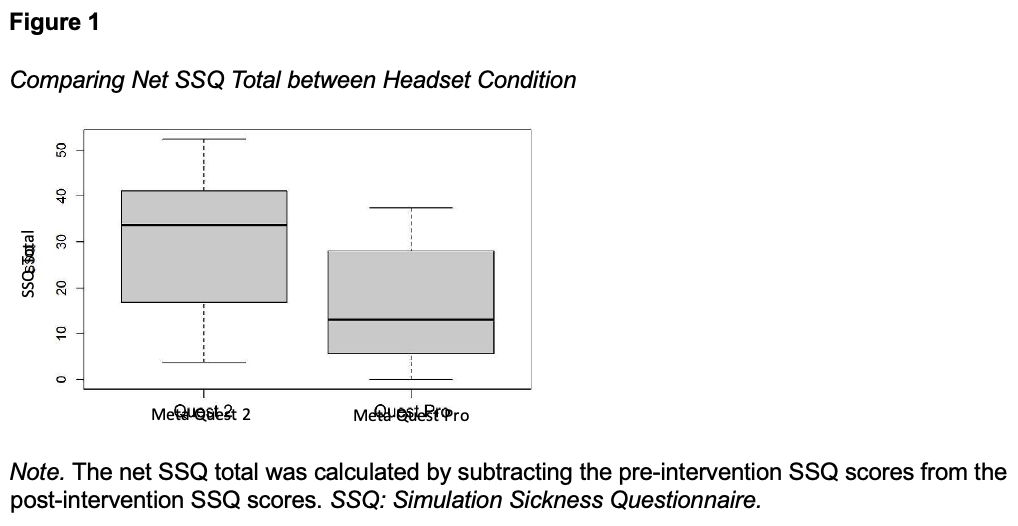
Data from the VIMSSQ, MSSQ, and discomfort dial were collated and de-identified. Statistical analysis was performed in RStudio (R Core Team, 2023). The net SSQ total was calculated by subtracting the pre-intervention SSQ scores from the post-intervention SSQ scores. The same process was repeated for the nausea, oculomotor, and disorientation components of the SSQ.
Ordinary least squares regression analysis was performed comparing VIMSSQ score, MSSQ score, gender, headset condition, and IPD mismatch in millimeters with the net SSQ total, the nausea component of the SSQ score, the oculomotor component of the SSQ score, the disorientation component of the SSQ score, the onset of discomfort, the average discomfort level, and the average peak discomfort level. All regressions were evaluated using robust standard error type HC1 and evaluated against diagnostic tests of assumption. Two observations were identified during analysis as significant outliers and removed from the dataset. This resulted in 32 total observations, with 16 from the Meta Quest 2 group and 16 from the Meta Quest Pro group.
Results
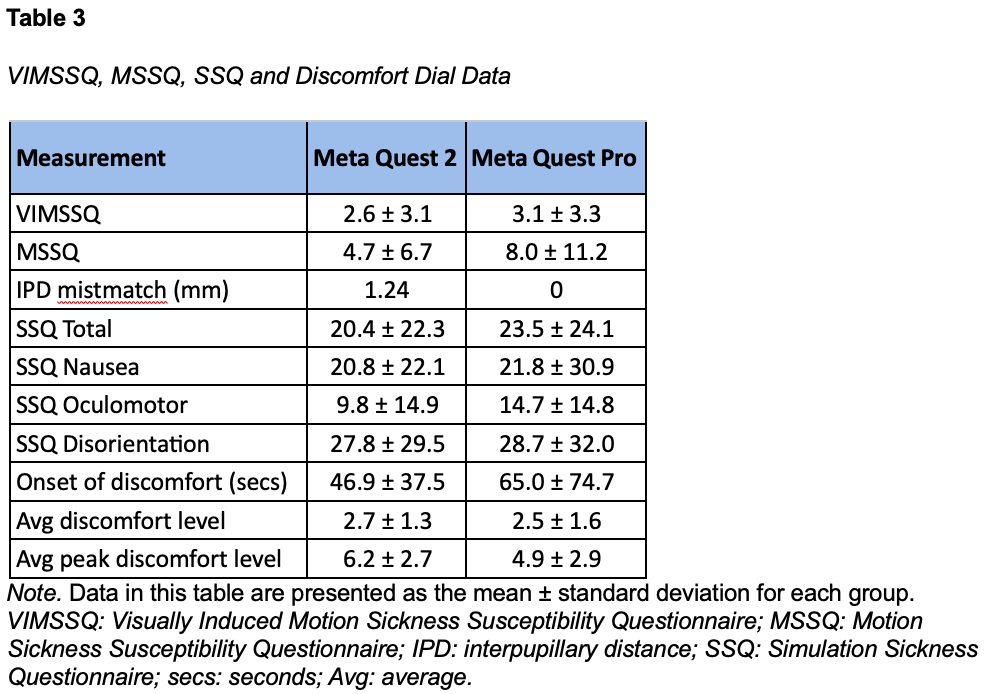
For each group, the average of the VIMSSQ, MSSQ, IPD mismatch, net SSQ Total, and SSQ components is presented in Table 3. Additionally, Table 3 includes data collected from the discomfort dial, such as the onset of discomfort, average discomfort level, and average peak discomfort levels for each group.
VIMSSQ
VIMSSQ scores demonstrated no significant relationship to the net SSQ total, SSQ component scores, discomfort onset time, or average discomfort level. For every one-unit in VIMSSQ score, the average peak discomfort level is predicted to increase by 0.28 units (95% CI: 0.002-0.558, p = 0.044, R2 = 0.25), controlling for age, gender, headset type, and IPD mismatch.
MSSQ
The MSSQ score demonstrated no significant relationship to the net SSQ total, SSQ component scores, onset of discomfort, average discomfort level, or average peak discomfort level.
Gender
Gender demonstrated no significant relationship to the net SSQ total, SSQ component scores, onset of discomfort, average discomfort level, or average peak discomfort level.
Headset Condition
The headset condition, either Meta Quest 2 or Meta Quest Pro, demonstrated no significant relationship to SSQ component scores, onset of discomfort, average discomfort level, or average peak discomfort level. However, it did exhibit a significant effect on the net SSQ total. The use of the Meta Quest Pro headset is predicted to decrease the net SSQ total by 11.24 points (95% CI: 1.27-21.2, p = 0.03, R2=0.15) when ignoring all other independent variables (Figure 1). No significant interactions were noted with gender.
IPD Mismatch
The average IPD mismatch for the Meta Quest 2 group was 1.24 millimeters with a range of -2 to +2 millimeters. Because the Meta Quest Pro allows for continuous IPD adjustment within the range of 55-75 millimeters, no participants in the Meta Quest Pro group had a mismatch between their IPD measurement and the IPD setting of the device.
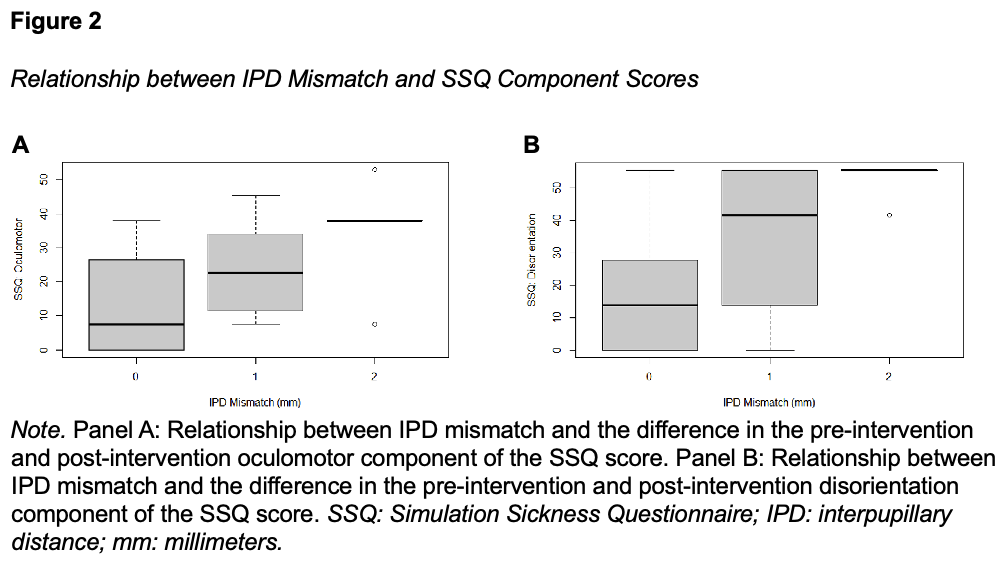
The IPD mismatch in millimeters demonstrated no significant relationship to the net SSQ total, nausea component of the SSQ score, onset of discomfort, average discomfort level, or average peak discomfort level. However, there was a significant relationship between IPD mismatch in millimeters and both the oculomotor and disorientation components of the SSQ score. For every 1-millimeter increase in the absolute mismatch between the participant’s IPD and the IPD setting of the headset, the difference between the pre-intervention and postintervention oculomotor component of the SSQ score was predicted to increase by 14.63 points (95% CI: 4.3-25.0, p=0.01, R2 =0.35), controlling for age, gender, and headset model (Figure
2A). Similarly, for every 1-millimeter increase in the absolute mismatch between the participant’s IPD and the IPD setting of the headset, the difference between the pre-intervention and postintervention disorientation component of the SSQ score was predicted to increase by 24.86 points (95% CI: 11.5-38.2, p<0.001, R2=0.44), controlling for age, gender, and headset model (Figure 2B). The correlation between the headset condition and IPD mismatch variables was observed to be 0.76. Removing the headset condition as an independent variable predicted a 12.04-point increase (95% CI: 5.42-18.65, p<0.001, R2=0.34) in the oculomotor component of the SSQ score and a 17.32-point increase (95% CI: 8.50-26.13, p<0.001, R2=0.39) in the disorientation component for every one-unit increase in IPD mismatch, controlling for gender and age.
Discussion
In this study, we evaluated the relationships between VIMSSQ score, MSSQ score, gender, headset condition, and IPD mismatch on the SSQ total score, SSQ component scores, onset of discomfort, average discomfort level, or average peak discomfort level. While MSSQ score and gender exhibited no significant effect, a relationship was noted between the VIMSSQ score and the average peak discomfort level. An increase of one unit in the VIMSSQ score is predicted to result in a 0.28-point rise in the peak discomfort level. For instance, a participant with a VIMSSQ score of 8 would be expected to have a peak discomfort level that is 1.4 points, or 14%, higher than that of a participant with a VIMSSQ score of 3. The short amount of time required to complete the VIMSSQ and relevance to predicting peak discomfort may provide some utility in identifying participants at risk for increased cybersickness symptoms before they engage in a VR simulation.
Additionally, the headset condition and IPD mismatch exhibited significant effects. Prior studies have identified female gender as contributing to the incidence of cybersickness (Biocca, 1992; Clemes & Haworth, 2005). More recent studies found gender to not be influential on cybersickness (Davis, Nesbitt, & Nalivaiko, 2014; Melo, Vasconcelos-Raposo, & Bessa, 2018). Stanney et al. (2020) discovered that while gender had a significant main effect on the development of cybersickness in a high-intensity roller-coaster simulation, the primary factor driving increased cybersickness in females was IPD mismatch. This study noted the HTC Vive headset used had an IPD range of 60.5 - 74.4 mm. This range would not fit approximately 35% of Asian, Caucasian, and African American females. The results of our study seem consistent with findings demonstrating no main effect of gender, but a significant contribution of IPD mismatch to the oculomotor and disorientation components of the SSQ score (Figure 2).
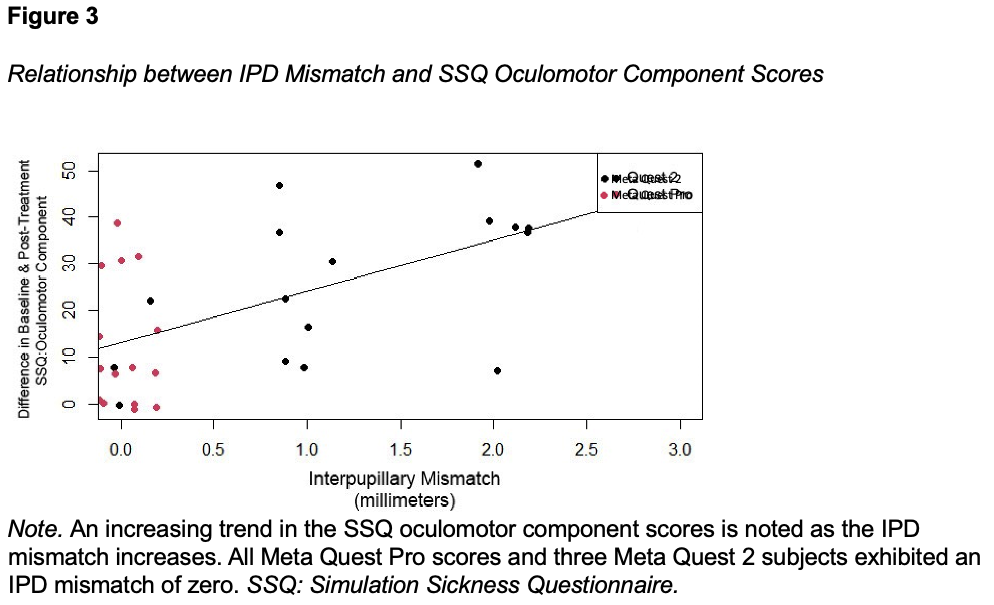
Because the Meta Quest 2 has only three IPD settings, only three of the sixteen participants included in the analysis for the Meta Quest 2 had a perfect IPD fit (Figure 3). Seven participants exhibited an IPD mismatch of 1 mm and six exhibited an IPD mismatch of 2 mm. In contrast, the Meta Quest Pro has an IPD range of 55-75 mm. Because of the larger range and capability of continuous adjustment, all participants using the Meta Quest Pro had a headset IPD setting that exactly matched their measured IPD. It must be considered that the accuracy of IPD adjustment could be a significant contributing factor in the lower SSQ scores associated with the Meta Quest Pro headset in at least some persons. Knowing one’s own IPD and ensuring that the headset is set appropriately could result in decreased symptoms.
At the time of this writing, Meta has discontinued the Meta Quest Pro in favor of the less expensive Meta Quest 3, priced at $499. The Meta Quest 3 retains the occlusive goggle design of the Meta Quest 2 but offers several improvements over the Meta Quest Pro. It has a higher resolution of 2064 x 2208 compared to 1800 x 1920, a faster refresh rate of 120 Hz vs 90 Hz, and a wider horizontal field of view of 110 degrees vs 106 degrees. Additionally, it is 28% lighter (Meta Quest Pro Vs Meta Quest 3 (Comparison) - VRcompare, 2023). Although the Meta Quest 3 retains the continuous IPD adjustment, it decreases the IPD range from 55-75 millimeters down to 58-71 millimeters. In this study, subjects using the Meta Quest Pro experienced an IPD mismatch of zero. However, if the Meta Quest 3 had been used, three subjects (18.8%) would have experienced an IPD mismatch of 1 mm.
Limitations
The small sample size used in this research presents a limitation to the interpretation of findings. Similarly, the use of a convenience sample of nursing students at a single university in the southeast United States could limit the generalizability of the results to other populations. Finally, other characteristics of the Meta Quest Pro not evaluated in this study which could influence the SSQ score include the following: higher frame rate, lower latency, comfort-related design features such as balanced front-to-back weight distribution and open goggle design.
Conclusion
In this study, VIMSSQ scores proved of use in predicting the peak symptoms experienced in a roller-coaster simulation. The Meta Quest Pro headset demonstrated a notable reduction in cybersickness as measured by the total SSQ score. More significantly, it appears that the wide range and accuracy of the IPD adjustment of the Meta Quest Pro headset contributed to significant decreases in the oculomotor and disorientation components of the SSQ score. As researchers consider implementing VR headsets, it would be prudent to evaluate the IPD adjustability of the headset. Comparing this with the average IPD range of the population may help to reduce the contribution of IPD mismatch on the severity and incidence of cybersickness.