Lith Nasif, MD1; Anna Hendricks, MD1; Elizabeth Harvey, MD2; Kirk Atkinson3; Ngoc Van Horn, MD1
1University of Texas Southwestern, Department of Pediatrics, Dallas, TX
2Texas Children’s Hospital, Department of Urgent Care, Houston, TX
3Universit of Texas Southwestern, UT Southwestern Simulation Center, Dallas, TX
Corresponding Authors
Lith Nasif (email: lith.nasif@utsouthwestern.edu); Ngoc Van Horn (email: ngoc.vanhorn@utsouthwestern.edu)
SUMMARY
Introduction: Nasal and otic foreign bodies are common in pediatric practice, but most trainees have limited procedural experience because of inconsistent patient availability and safety concerns. Commercial task trainers are often expensive or lack pediatric anatomical realism. Lowcost 3D printing offers an accessible alternative; however, there are few published models that address foreign body removal. This activity used a 3D-printed pediatric head to determine whether a low-cost task trainer could improve learner comfort and knowledge with foreign body removal.
Methods: Participants included 28 incoming pediatric interns at a large academic medical center. Learners completed a pre-simulation survey that gauged experience, comfort, and procedural knowledge. Trained pediatric residents facilitated learners through otic and nasal foreign body removal using otoscopes, alligator forceps, hooks, and Katz extractors on a 3D-printed task trainer. After practice, participants completed a post-simulation survey assessing comfort and knowledge. Knowledge improvement was measured using a multiple-choice quiz; comfort was measured using a Likert scale. Paired t-tests were used to determine significance between pre- and post-simulation knowledge scores and comfort.
Results: At baseline, 64% of participants reported no prior exposure to foreign body removal, and 60% indicating they were “not comfortable at all.” Knowledge scores improved from 48% pre-simulation to 95% post-simulation (p < 0.001). Similarly, comfort improved significantly, with 65% of participants reporting readiness to perform the procedure with minimal assistance (p < 0.01).
Conclusion: This low-cost 3D-printed task trainer is an effective method of enhancing learner confidence and procedural knowledge. Its affordability and reproducibility support broad implementation, particularly in resource-limited educational settings.
INTRODUCTION
Foreign body insertion into the ears and nose is a common occurrence in pediatric populations, frequently leading to evaluations, either outpatient or in the emergency department (DiMuzio & Deschler, 2002; Heim & Maughan, 2007). While most foreign bodies can be safely removed in minimally resourced clinical settings, unsuccessful attempts may result in complications such as mucosal injury, bleeding, infection, or aspiration (Schulze et al., 2002). Early and effective management is, therefore, essential. As per the procedures list in the ACGME Entrustable Professional Activities 1: “All pediatricians must be familiar with appropriate simple foreign body removal techniques and instrumentation prior to graduation” (The American Board of Pediatrics, 2021).
Despite the frequency of these cases, many pediatric trainees receive limited hands-on experience with foreign body removal prior to encountering it in clinical practice. Traditional opportunities for procedural education in this area are often inconsistent, dependent on patient availability, and constrained by patient safety concerns (Barsuk et al., 2012). Simulation-based education offers a valuable alternative by providing trainees with a safe and controlled environment without feeling the constraints of patient fear, parental anxiety, or timing. This encourages learners to explore, reflect, and develop procedural confidence before performing these skills on patients (Okuda et al., 2009).
Although several task trainers for ear and nasal foreign body removal exist, commercially available models are often expensive, lack anatomical accuracy, or do not allow for repeated use (Sawyer et al., 2015). Advances in three-dimensional (3D) printing technology have created opportunities for low-cost, customizable, and reproducible simulation tools that can enhance procedural training in resource-limited environments (Weinstock et al., 2017).
In this study, we describe the design and implementation of a low-cost, 3D-printed pediatric task trainer for otic and nasal foreign body removal. We also evaluate its educational value through pre- and post-simulation assessments of trainee comfort and knowledge. Our goal is to provide an accessible, reproducible model that can be used to improve pediatric procedural education in diverse training settings.
METHODS Manufacturing of Head
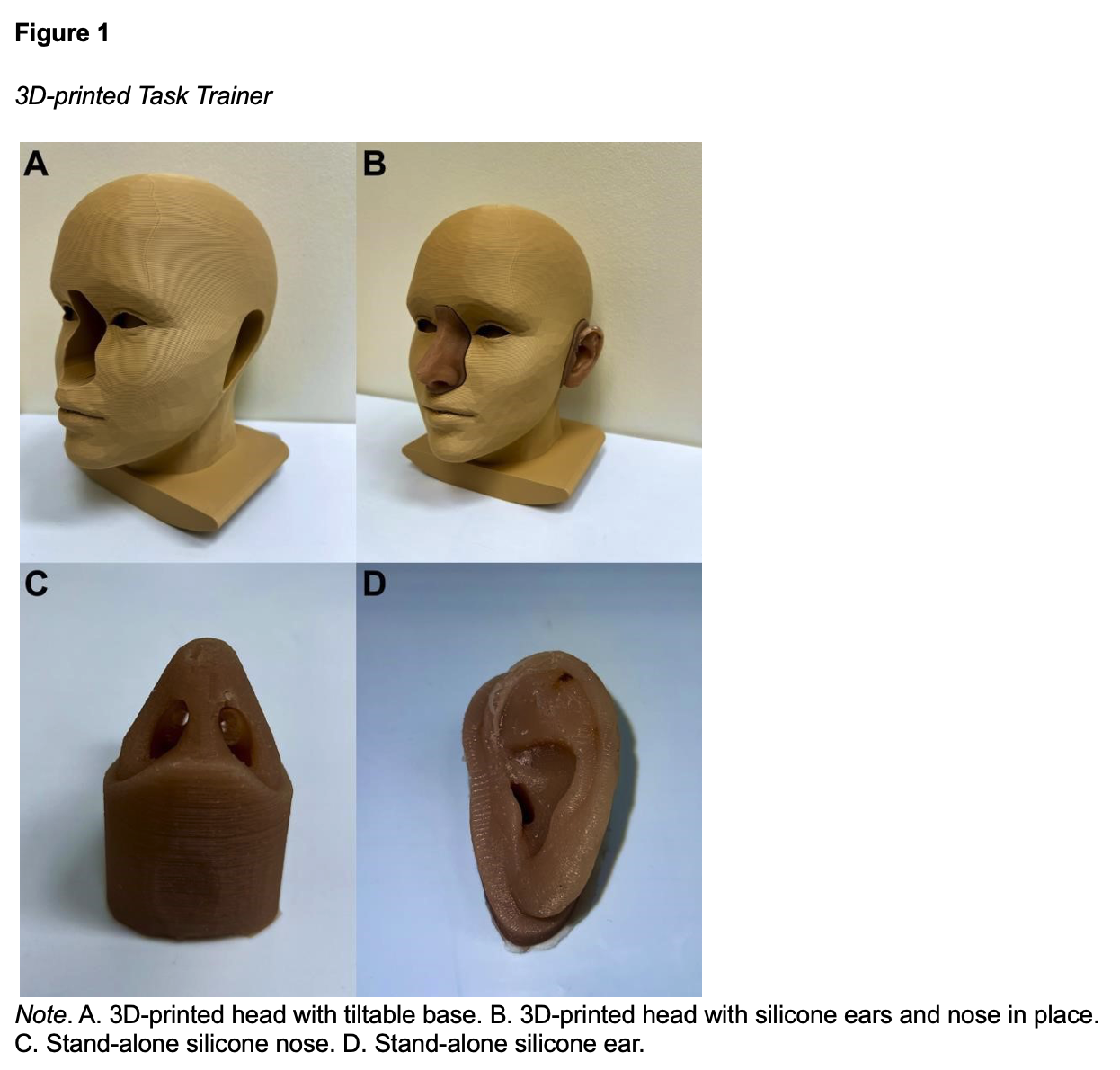
A 3D model of a pediatric head was obtained from an open-access online design database (Head, 2015). Fusion 360 design software (v.2605.0.97; Autodesk Fusion, 2025) was then used to modify the design, including sizing the model according to average dimensions of a 5-year-old child, adding a tiltable base, and incorporating removable ear and nose pieces (World Health Organization, n.d.). The base was adjusted to achieve a balance of stability and maneuverability in the horizontal axis based on feedback from users. The ears were designed to simulate a 5-year-old child’s ear by incorporating a hole behind the tragus in the shape of an ellipse with a major axis of 10mm, a minor axis of 5mm, and a depth of 15mm (Voss et al., 2025). Similarly, the nose was designed to simulate bilateral nares connecting at the nasopharynx by including two elliptical openings with a major axis of 10mm, a minor axis of 6.5mm, and a total depth of 50mm (3D-Printed Task Trainer for Pediatric Otic & Nasal Foreign Body Removal, 2025; Zalzal et al., 2018).
The head and base design (which did not include the ears and nose) was sliced using Bambu Slicer software (v2.0.3; Bambu Studio, 2025). It was printed on a Bambu P1S printer with a 0.6 mm nozzle using light brown matte PLA filament. Standard print settings were used, except for a layer height of 0.38 mm, 3 wall loops, 10% infill, and tree support. The total print time was 15 hours and 30 minutes, and it required 703 grams of PLA filament.
The ears and nose were made using molds formed from 3D-printed negative models of the ears and nose/nostrils. The STL files are available for download (3D-Printed Task Trainer for Pediatric Otic & Nasal Foreign Body Removal, 2025). Both the molds and negative models were sprayed with a release agent to prevent adhesion to the mold. Ecoflex 00-30 silicone was measured, pigmented, mixed, and poured into the molds to cover the negative models. After curing for 4 hours, the silicone components were removed from the molds. For the nasal pieces, the 3D-printed nostril inserts remained embedded in the silicone. A small incision was made at the superior anatomical aspect of the nose model to allow removal of the internal negative insert. Excess silicone was carefully trimmed from the model. The ear and nose models snap into the head model without the use of any adhesives (Figure 1).
Task Trainer Facilitation Protocol and Survey Questions
Incoming pediatric interns at the University of Texas Southwestern, a large academic graduate medical program, participated in a multi-station procedural and simulation bootcamp. One station focused on pediatric foreign body removal, using the above task trainer. The simulation was facilitated by trained pediatric residents, chosen by a board-certified pediatrician. Facilitators utilized a standardized script that discussed the prevalence of ear and nose foreign bodies in the pediatric setting, highlighted methods for removal of various types of foreign bodies, including organic, inorganic, and insects, as well as indications for subspecialty consultation (Appendix A).
After a brief explanation of the purpose of the station, participants were asked to complete a pre-simulation survey, which assessed comfort, knowledge, and previous experience with foreign body removal (Appendix B). Participants first practiced the removal of inorganic foreign bodies (beads) from the silicone ears using an otoscope, alligator hook, and forceps. They were then able to complete hands-on practice with the nose model to remove foreign bodies using a Katz extractor. The procedural facilitator assisted with the simulation, ensured critical actions were performed, and was available to answer questions. The participants were given about five minutes at the station to practice foreign body removal.
After completing the simulation, all participants were given a post-simulation survey (Appendix B) to assess their confidence and knowledge related to foreign body removal. A knowledge-based quiz was developed from the procedure’s critical actions and aligned with the stated learning objectives. The content was reviewed and approved by a separate team of procedural experts. The quiz consisted of multiple-choice questions addressing key steps and management strategies for the removal of different types of foreign bodies (bead, popcorn, and insect).
Data Analysis
Survey results were compiled and organized in Microsoft 365 Excel (version 16.0). Paired ttests were used to compare pre- and post-simulation comfort scores and percentage of correct responses on the knowledge assessment. P-values less than < 0.05 were considered statistically significant.
RESULTS
Twenty-eight pediatric interns participated in the foreign body removal using the task trainer and completed both the pre- and post-simulation surveys. The majority of participants (64%) had no previous experience observing or performing foreign body removal, 29% of participants reported observing the procedure, and only 7% of respondents reported any hands-on experience with the procedure (Figure 2).
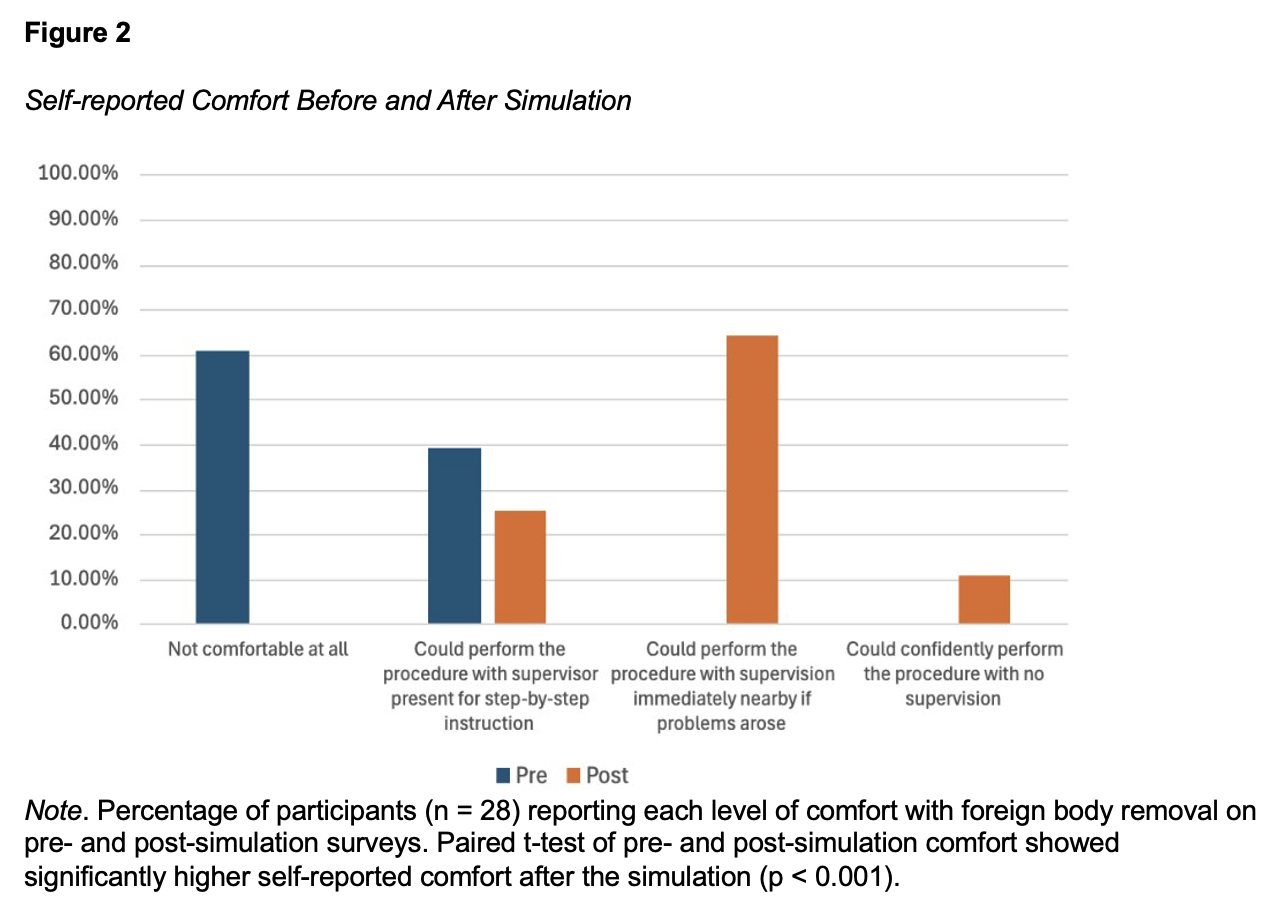
On the pre-simulation survey, 60% of participants indicated that they were not comfortable at all with foreign body removal and would prefer to watch someone demonstrate the entire procedure for them before attempting it with a real patient. After completing the station, 65% of participants felt they could complete the procedure, as long as help was nearby if problems arose (Figure 2). Similarly, participants felt significantly more comfortable with the procedure when comparing selfreported comfort on the pre-simulation survey (M = 1.39, SD = 0.50) to the post-simulation survey (M = 2.86, SD = 0.59, p < 0.001). For knowledge, participants scored significantly higher on the postsimulation assessment (M = 2.86, SD = 0.36, p < 0.001) than on the pre-simulation assessment (M = 1.46, SD = 0.64).
DISCUSSION
These results suggest that our low-cost, 3D-printed task trainer for otic and nasal foreign body removal is an effective educational tool to improve both trainee comfort and knowledge. Our subjects, a cohort of incoming pediatric interns, had a critically low baseline level of experience, with less than 10% having prior hands-on exposure to foreign body removal. This reinforces existing literature, which highlights inconsistency in traditional, patient-dependent procedural training. After a standardized simulation session, self-reported comfort levels and objective knowledge both improved significantly, with the average knowledge assessment score rising from 48% to over 95%. These results align with the use of simulation-based education in medicine, which creates a safe and repeatable environment necessary to build procedural competence and confidence (Okuda et al., 2009).
A key strength of this task trainer is its use of 3D printing technology to develop an accessible and reproducible model. Commercial simulation models are often very expensive, creating a significant barrier in resource-limited or global health contexts (Weinstock et al., 2017). For example, an ear examination simulator, with a similar design to our 3D printed task trainer, costs over $1,300 (Ear Examination Simulator, n.d.).
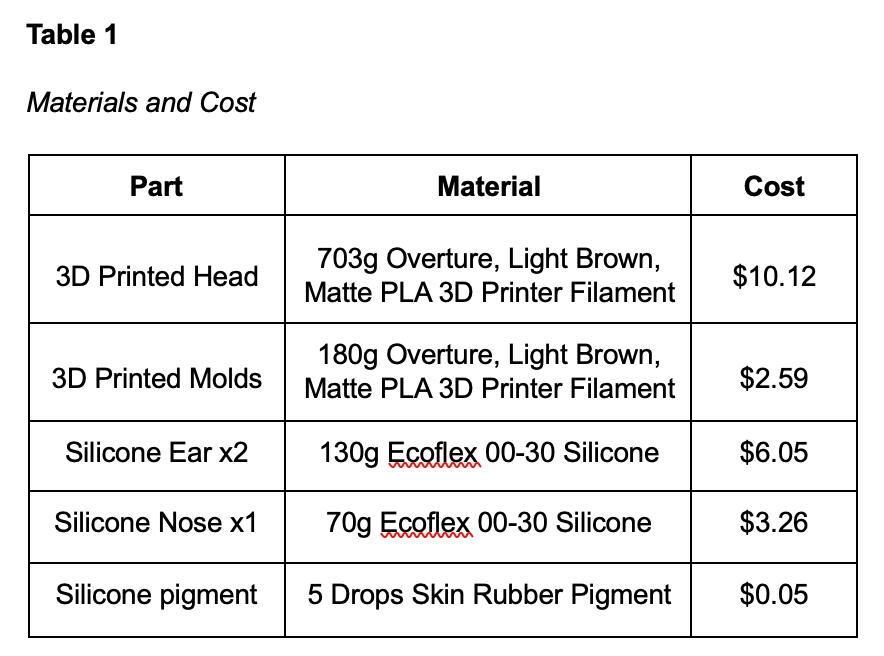
Multiple iterations of the task trainer were attempted and revised based on user feedback to make the most user-friendly and realistic version possible. The two main adjustments to the initial prototypes were the tiltable base and the material for the ears and nose. The base was initially larger and gave less opportunity to tilt, but this was improved in the current design. Initially, the ears and nose were 3D printed with flexible TPU material, but user feedback indicated that it was not flexible enough. As a result, we switched to silicone casting. We used open-source digital models and inexpensive PLA filament and silicone to create a trainer with a materials cost under $25 using a commercial 3D printer. The task trainer has also proven to be durable, with no signs of wear on the ears or nose after more than 50 users. When damage does occur, the ears and nose can be replaced for about $3 (Table 1). This approach aligns with the increased use of additive manufacturing in medical education to create customizable for procedural practice (Weinstock et al., 2017). Additionally, the low production cost makes this model feasible for mass distribution and helps address challenges in procedural skill development in underserved areas (Olatunji et al., 2023).
Limitations
Future research is needed to validate the clinical utility of this model and test participants’ ability to apply the skills learned to actual patient care. This study had several limitations, including that it was performed at a single academic center with a small cohort of participants, which may limit the generalizability of our findings. Additionally, participant comfort was self-reported and a subjective assessment. More importantly, this study only accounted for immediate post-simulation of knowledge and comfort, and it did not test knowledge retention over time.
Future Research
Future developments in this space could include designing a comprehensive line of 3D printable, open-source task trainers to support a simulation curriculum in under-resourced areas, making simulation accessible to trainees worldwide. Although our study has laid out the framework for designing, manufacturing, and using 3D printable task trainers, additional, larger-scale and longitudinal studies are needed to make 3D printable simulation models a standard part of medical education.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Acknowledgements: The authors would like to acknowledge the UT Southwestern Simulation Center for providing the resources, personnel, and support necessary to conduct this research.
Please cite this article as: Nasif, L., Hendricks, A., Harvey, E., Atkinson, K., & Van Horn, N. (2026). A low-cost 3D-printed task trainer for pediatric otic & nasal foreign body removal. Simulation Technology & Operations Resource Magazine, 5(2), 34-43. ISSN: 3070-3506.
REFERENCES
3D-Printed Task Trainer for Pediatric Otic & Nasal Foreign Body Removal. (2025, November 29). Thingiverse. Retrieved November 29, 2025, from https://www.thingiverse.com/thing:7214965
Barsuk, J. H., Cohen, E. R., Caprio, T., McGaghie, W. C., Simuni, T., & Wayne, D. B. (2012). Simulation-based education with mastery learning improves residents’ lumbar puncture skills. Neurology, 79(2), 132–137. https://doi.org/10.1212/wnl.0b013e31825dd39d
DiMuzio, J., & Deschler, D. G. (2002). Emergency Department management of foreign bodies of the external ear canal in children. Otology & Neurotology, 23(4), 473–475. https://doi.org/10.1097/00129492-200207000-00014
Ear Examination Simulator. (n.d.). 3B Scientific. Retrieved November 22, 2025, from https://www.3bscientific.com/us/ear-examination-simulator-1005645-w44122-nascolf01019,p_1457_4994.html
Head. (2015, August 22). Thingiverse. Retrieved November 22, 2025, from https://thingiverse.com/thing:979818/makes
Heim, S., & Maughan, K. (2007). Foreign bodies in the ear, nose, and throat. American Family Physician, 26(8), PMID: 17990843.
Okuda, Y., Bryson, E. O., DeMaria, S., Jacobson, L., Quinones, J., Shen, B., & Levine, A. I. (2009). The utility of simulation in medical Education: What is the evidence? Mount Sinai Journal of Medicine a Journal of Translational and Personalized Medicine, 76(4), 330–343. https://doi.org/10.1002/msj.20127
Olatunji, G., Osaghae, O. W., & Aderinto, N. (2023). Exploring the transformative role of 3D printing in advancing medical education in Africa: a review. Annals of Medicine and Surgery, 85(10), 4913–4919. https://doi.org/10.1097/ms9.0000000000001195
Sawyer, T., White, M., Zaveri, P., Chang, T., Ades, A., French, H., Anderson, J., Auerbach, M.,
Johnston, L., & Kessler, D. (2015). Learn, see, practice, prove, do, maintain. Academic Medicine, 90(8), 1025–1033. https://doi.org/10.1097/acm.0000000000000734
Schulze, S. L., Kerschner, J., & Beste, D. (2002). Pediatric External Auditory Canal Foreign Bodies: A review of 698 cases. Otolaryngology, 127(1), 73–78. https://doi.org/10.1067/mhn.2002.126724 The American Board of Pediatrics. (2021). Entrustable professional activities for general pediatrics. Retrieved November 22, 2025, from https://www.abp.org/sites/abp/files/pdf/combined_gp_epas.pdf
Voss, S. E., Remenschneider, A. K., Farrar, R. M., Myoung, S., & Horton, N. J. (2025). Comprehensive measurements and analyses of ear canal geometry from late infancy through late adulthood: Age-Related Variations and implications for basic science and audiological measurements. Trends in Hearing, 29, 23312165251345572. https://doi.org/10.1177/23312165251345572
Weinstock, P., Rehder, R., Prabhu, S. P., Forbes, P. W., Roussin, C. J., & Cohen, A. R. (2017). Creation of a novel simulator for minimally invasive neurosurgery: fusion of 3D printing and special effects. Journal of Neurosurgery: Pediatrics, 20(1), 1-9. https://doi.org/10.3171/2017.1.PEDS16568
World Health Organization. (n.d.). Head circumference-for-age Boys. Retrieved November 22, 2025, from https://cdn.who.int/media/docs/default-source/child-growth/child-growth-
Zalzal, H. G., O’Brien, D. C., & Zalzal, G. H. (2018). Pediatric anatomy: nose and sinus. Operative Techniques in Otolaryngology-Head and Neck Surgery, 29(2), 44–50. https://doi.org/10.1016/j.otot.2018.03.002
Appendix A
Foreign Body Removal Facilitator Guide
Complete Pre-Simulation Survey
General Intro
Discuss prevalence of procedure: 45,000 ER visits annually for just ear foreign bodies.
Discuss importance of training: Removal success highest on first attempt
Ear Canal
Always perform otoscopy first to evaluate the foreign body and the tympanic membrane (What is the object? Is the TM intact?)
Discuss positioning: sitting or semi-reclined, consider need for restraints (wrap arms / legs), distraction (child life, tablet), sedation needed?
Irrigation is good first step for small inorganic objects o Fill a 30- to 60-mL syringe with sterile water warmed to body temperature.
Inject a stream of water into the superior aspect of the external canal behind the foreign object using moderate pressure, with a kidney basin under the ear to catch water.
Do NOT use irrigation if:
Object is soft or might swell if water added (i.e. bean, popcorn, seed)
Object is button battery or magnet, as water may accelerate damage
Known or suspected perforation of tympanic membrane for FB in the ear
Manual instrumentation is good for wide variety of objects such as cotton tips, button batteries, and large beads o Insert a right-angle hook or loop and insert the instrument to the edge of the object under direct visualization.
Slip the instrument behind the object and gently pull it out of the canal
Nostril
Katz extractor is often the best first option.
Insert the extractor past the object. Inflate with 1 mL of air using the attached syringe. Remove the extractor and the foreign body from the canal with balloon inflated.
Can also attempt positive pressure by keeping opposite nostril occluded and having patient blow forcefully. Not always possible based on age / cooperation level.
Special Considerations (discuss if time permits)
For living foreign bodies (i.e. insects):
Tilt the affected ear upward. Use a dropper to fill the ear canal with warm mineral oil or lidocaine solution. Wait 1-2 minutes to kill the insect and numb the canal.
Gently grasp the body, wing, or leg of the insect with alligator forceps and gently pull the entire insect out of the ear.
Consult ENT for:
Posterior nasal foreign bodies (cannot see from looking into nares anteriorly) o Impacted foreign bodies with marked inflammation or penetrating FB
Evidence of vestibular symptoms (nausea, vomiting, nystagmus, vertigo, or ataxia)
Appendix B
Foreign Body Removal Learning Objectives
By the end of this session, learners will be able to:
Identify appropriate tools (e.g., suction, forceps, hooks) based on foreign body type and location (ear canal vs. nostril)
Practice safe foreign body extraction with minimal damage in a simulated environment
Adapt techniques for common scenarios: organic materials (e.g., food) vs. inorganic objects (e.g., beads, batteries) vs. living specimens (e.g., insects)
Demonstrate knowledge and perceived comfort level via post-simulation surveys
Foreign Body Removal Pre-Simulation Survey
Have you previously observed or performed a foreign body removal?
Yes, observed only
Yes, performed with supervision
Yes, performed independently
No experience
How comfortable do you feel removing any foreign body from a pediatric patient’s ear or nose?
Not comfortable at all, I would prefer to watch someone demonstrate the entire procedure for me.
I could perform the procedure if a supervisor were present to give hands-on, step-bystep instruction.
I could perform the procedure with supervision immediately nearby (i.e. available outside the room or down the hallway) if problems arose.
I could confidently perform the procedure independently with no supervision.
Which of the following is the most appropriate method to remove a firm, inorganic foreign body (e.g. a plastic bead) from a child’s ear?
Use water irrigation, a Katz extractor, or a right-angle hook, based on the object’s characteristics.
Instill mineral oil and wait for the object to soften or dissolve.
Instruct the patient to blow their nose while occluding the opposite nostril.
Insert a balloon syringe-catheter (Katz extractor) without visualizing the full extent of the object.
How would you remove an organic foreign body (i.e. a piece of popcorn) from a nostril?
Use a Katz extractor or a right-angle hook, based on the object’s characteristics.
Use water irrigation with a syringe and sterile saline to flush the object out of the nostril.
Apply tissue adhesive to a cotton swab and stick it to the object before slowly removing it.
Instill mineral oil and wait for the object to soften or dissolve before attempting removal.
What would be your first step in removing a living foreign body (i.e. a bug) from an ear?
Instill mineral oil into the ear canal before removal to immobilize the insect.
Immediately attempt to remove with forceps to ensure quickest removal of the insect.
Use water irrigation to flush the insect out of the ear canal.
Ask the patient to blow their nose forcefully while occluding the opposite nostril.
Foreign Body Removal Post-Simulation Survey
After participating in the foreign body removal procedural station, how comfortable do you feel removing a foreign body from a pediatric patient’s ear or nose?
Not comfortable at all, I would prefer to watch someone demonstrate the entire procedure for me.
I could perform the procedure if a supervisor were present to give hands-on, step-bystep instruction.
I could perform the procedure with supervision immediately nearby (i.e. available outside the room or down the hallway) if problems arose.
I could confidently perform the procedure independently with no supervision.
Which of the following is the most appropriate method to remove a firm, inorganic foreign body (e.g. a plastic bead) from a child’s ear?
Use water irrigation, a Katz extractor, or a right-angle hook, based on the object’s characteristics.
Instill mineral oil and wait for the object to soften or dissolve.
Instruct the patient to blow their nose while occluding the opposite nostril.
Insert a balloon syringe-catheter (Katz extractor) without visualizing the full extent of the object.
How would you remove an organic foreign body (i.e. a piece of popcorn) from a nostril?
Use a Katz extractor or a right-angle hook, based on the object’s characteristics.
Use water irrigation with a syringe and sterile saline to flush the object out of the nostril.
Apply tissue adhesive to a cotton swab and stick it to the object before slowly removing it.
Instill mineral oil and wait for the object to soften or dissolve before attempting removal.
What would be your first step in removing a living foreign body (i.e. a bug) from an ear?
Instill mineral oil into the ear canal before removal to immobilize the insect.
Immediately attempt to remove with forceps to ensure quickest removal of the insect.
Use water irrigation to flush the insect out of the ear canal.
Ask the patient to blow their nose forcefully while occluding the opposite nostril.
What feedback do you have for this task-trainer and/or procedure station?