AUTHORS
Cheryl Camacho, MBA, CHSE-A, Paramedic, FSSH1; Ashley Brophy, MSN, PNP, CHSE2; Laura Valido, BSN, RN2; Rika Tanda, PhD, RN, CCRN3; Ahquilah Tucker, BSN, RN, CCRN2; Thomas Heater, RRT, BBA, CHSE1; Laura Beth Kalvas, PhD, RN4
1Center for Clinical Excellence Simulation Center, Nationwide Children’s Hospital, Columbus, OH
2Cardiothoracic Intensive Care Unit, Nationwide Children’s Hospital, Columbus, OH
3Respiratory Intensive Care Unit, Nationwide Children’s Hospital, Columbus, OH 4Center for Nursing Excellence, Nationwide Children’s Hospital, Columbus, OH
Corresponding Author
Cheryl Camacho, Cheryl.Camacho@nationwidechildrens.org
SUMMARY
The transition to critical care practice requires structured education to support clinical readiness among new graduate nurses. To standardize orientation across multiple Intensive Care Units (ICUs) and strengthen nurse competence, we developed and evaluated a multimodal, simulation-based ICU Core Curriculum utilizing scaffolded learning, didactic instruction, task training, and scenario-based simulation to promote critical thinking, skill acquisition, and interprofessional collaboration. The curriculum demonstrated an improvement in learner engagement, confidence, and knowledge in high-risk domains such as respiratory management and Code Blue response, while supporting adoption of evidence-based practices. Ongoing refinement through Plan-Do-Study-Act cycles and learner feedback, combined with consolidating orientation across multiple units and strategic use of simulation resources, resulted in significant cost savings, and demonstrated the value of a simulation-centered onboarding model.
BACKGROUND
Intensive Care Units (ICUs) are high-acuity environments requiring rapid clinical decision- making, advanced technical proficiency, and effective interprofessional collaboration. The evolving landscape of ICU nursing, shaped by increasingly complex patients, rapid technological advancement, and persistent staffing challenges, has amplified the urgency for effective onboarding strategies (American Association of Critical-Care Nurses, 2022). The ongoing shortage of experienced ICU nurses, compounded by retirement and turnover, has led to an experiencecomplexity gap, in which there is a disconnect between ICU patient acuity and readiness of novice nurses to safely manage their care. This places significant pressure on nurse educators and preceptors to bridge this gap and ensure safe, high-quality care. There is substantial financial pressure on healthcare organizations to onboard and retain critical care nurses. Estimates suggest the cost of onboarding a new graduate nurse can exceed $100,000 (Jones, 2021). More recent workforce analyses estimate the average cost of nurse turnover to be approximately $60,090 per nurse, with national nursing turnover rates averaging 17.6%, and turnover rates in ICU settings are reported to be even higher, averaging approximately 27% (Gamble, 2026).
In this context, simulation-based education emerges as a strategic solution to address the experience-complexity gap. Simulation training can significantly enhance learning and confidence for novice nurses transitioning into high-risk clinical settings (Rutherford-Hemming et al., 2022). A multimodal approach integrating instructional methods such as high-fidelity manikins, virtual reality, case-based discussions, and interprofessional team training can enhance learner engagement, promote critical thinking, and better prepare students for the complexities of clinical practice (Schwengel et al., 2025).
Our large Midwestern freestanding pediatric hospital has 72 ICU beds across three pediatric ICU’s: trauma, respiratory, cardiothoracic. Historically, each unit maintained separate orientation programs, resulting in inconsistent onboarding and inefficient resource utilization. To standardize competency development and orientation for newly hired nurses, ICU nurse educators collaborated with the hospital’s Simulation Center to develop and implement the ICU Core Curriculum, a multimodal, simulation-based program designed to provide consistent, evidence-based training across all ICU settings.
ICU Core Curriculum Development
The ICU Core Curriculum is a comprehensive approach to new-hire orientation in the ICU. A primary driver was the need to equip nurses with the requisite skills to deliver safe, coordinated, highquality care regardless of unit assignment. To address knowledge and performance gaps identified by ICU nurse educators, existing orientation lectures were supplemented with hands-on learning experiences, developed in collaboration with an interprofessional simulation team. The collaboration focused on enhancing learning strategies, improving educational delivery, and standardizing the onboarding process across units.
Our Simulation Center, accredited by the Society of Simulation in Healthcare (SSH), features diverse simulation modalities and immersive learning environments designed to replicate clinical practice. Simulation best practices are applied in curriculum design by Certified Healthcare Simulation
Educators (CHSE), ensuring that scenarios align with international standards (International Nursing Association for Clinical Simulation and Learning [INACSL], 2021a). Learners participate in small groups (≤ 7 per session) to maximize engagement, with each experience structured to include a formal prebrief, realistic simulation encounter, and debrief (INACSL, 2021a). Facilitators are trained in evidence-based debriefing methods and utilize Debriefing Assessment for Simulation in Healthcare scoring to promote reflection and skill integration (Al-Khayat et al., 2024).
We applied scaffold learning theory (INASCL, 2021a) to develop a week-long, progressive, multi-modal educational approach. Nurses attend the ICU Core Curriculum between weeks 10 and 12 of their 20-week orientation. Each day of the curriculum focuses on a specific area of patient care, such as respiratory or cardiovascular (Palmer et al., 2025). The morning didactic session includes interactive presentations with embedded polls and videos, open discussion using the Socratic method of teaching, and educational games. The afternoon session uses various simulation modalities to complement the didactic content. Examples include task training procedures, demonstrations with open discussion and return demonstration, scenario walkthroughs, low- and high-fidelity simulation cases, and escape rooms.
Based on the cognitive load associated with a week-long curriculum, careful consideration was placed on maintaining variety and balancing difficulty level to maintain learner engagement and transfer working memory to long-term memory. Additionally, the principles of Bloom’s Taxonomy (1956) were used to ensure learners were progressing in their level of learning from remembering to understanding, applying, and analyzing new knowledge (INASCL, 2021b). Careful consideration was given to a newer generation of adult learners who have unique educational learning needs and respond better to experiential learning (Masso et al., 2022). The ICU Core Curriculum agenda is provided below (Figure 1).
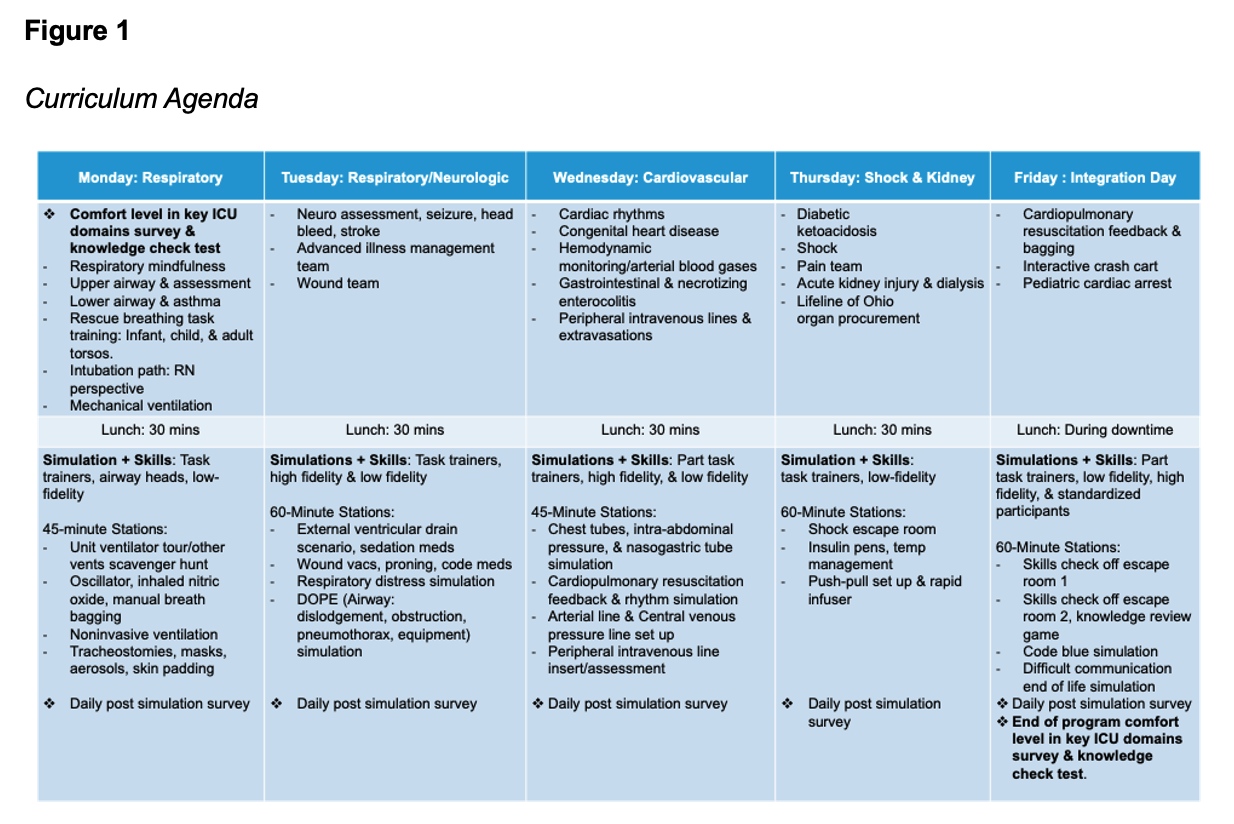
The agenda is one example of how the team incorporates Bloom’s Taxonomy (1956) and scaffolding learning in the objectives, simulation design, and strategic use of multimodal simulation (INASCL, 2021b). Day one is focused on respiratory education and exposure to various modes of simulation. Respiratory lectures define and describe assessments, blood gases, and mechanical support in preparation for the afternoon application stations and interactive ventilator escape room. In these breakouts, novice learners build on their understanding with faculty-supported hands-on application of devices, such as bilevel positive airway pressure (BiPAP), including setup, skin protection procedures, blood gas analysis, and device setting management. Airway heads and lowfidelity manikins are utilized to accomplish these learning objectives. The next afternoon, learners apply their respiratory knowledge during a respiratory distress simulation with a high-fidelity simulator. During the simulation, learners interpret blood gases and advocate escalating care, transitioning from nasal cannula to BiPAP. Each day of the curriculum follows this general simulation design.
The final training day is called Integration Day. It allows learners to synthesize the skills and knowledge refined throughout the week. Participants demonstrate their learning by rotating through several stations, including a knowledge check escape room, which encompasses the performance of skills practiced during the week.
PROGRAM EVALUATION
We assessed the program's effectiveness using surveys, tests, and cost analysis. Participant comfort in key ICU domains was assessed with a survey organized by body system (respiratory, cardiovascular, neurologic, hemodynamics) consistent with nursing professional development frameworks used in pediatric ICU onboarding (Palmer et al., 2025). Knowledge was assessed by an 11-item pre- and post-program test. Daily feedback was gathered utilizing the Simulation Center’s five-point Likert Scale and open-text simulation program survey to gauge skill improvement, likelihood of changing practice, and to provide feedback on the facilitator. Survey and test data were analyzed with descriptive statistics. Pre- and post-program data were compared using Mann-Whitney's test for the comfort scores and Fisher’s exact test for knowledge scores. The cost analysis was conducted through a retrospective review of training logistics and resource allocation prior to and following implementation of the ICU Core Curriculum.
The current ICU Core Curriculum is the result of continual improvements through Plan-Do- Study-Act (Zann, 2021) cycles of seven cohorts from 2023-2025. Changes were implemented based on participant program evaluation tests and surveys, faculty observations, and monthly standing educator meetings. Following the weekly implementation of the curriculum, the instructional team engaged in structured debriefing sessions. To critically examine the week’s teaching and learning experiences, these reflective meetings occurred promptly, while observations, student interactions, instructional outcomes, and survey results were still fresh in memory.
This process supported iterative improvements to both curriculum content and educational strategies, aligning with best practices in responsive and reflective teaching (Zann, 2021). Examples of iterative changes included adjusting the pacing and sequencing of respiratory content, increasing hands-on breakout time, refining simulation complexity, and standardizing facilitator prebriefing approaches. These modifications contributed to consistently high learner engagement, psychological safety, and perceived clinical preparedness across cohorts.
RESULTS
Between September 2023 and January 2025, 106 new-hire nurses participated in the ICU Core Curriculum.
Participant Comfort and Knowledge
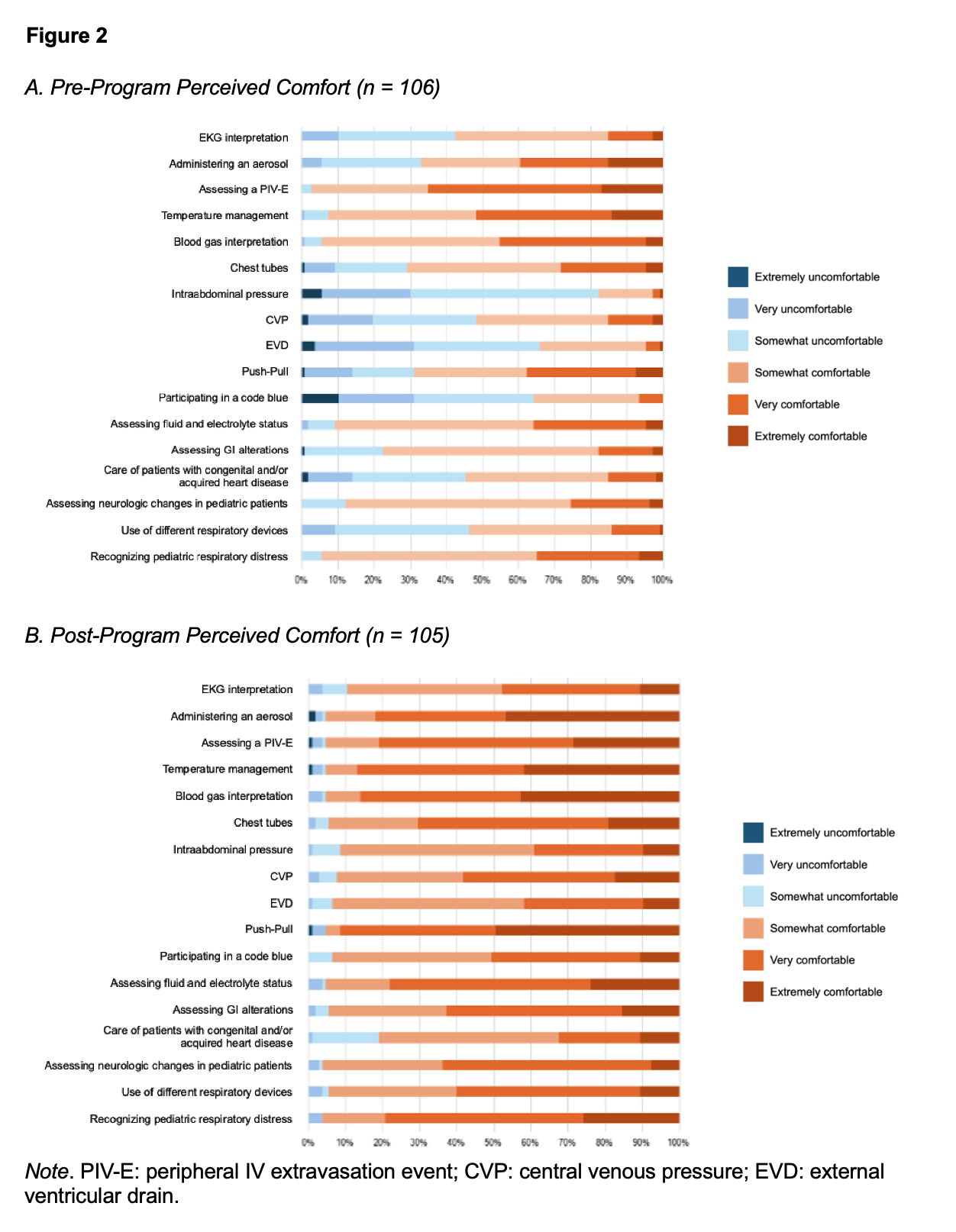
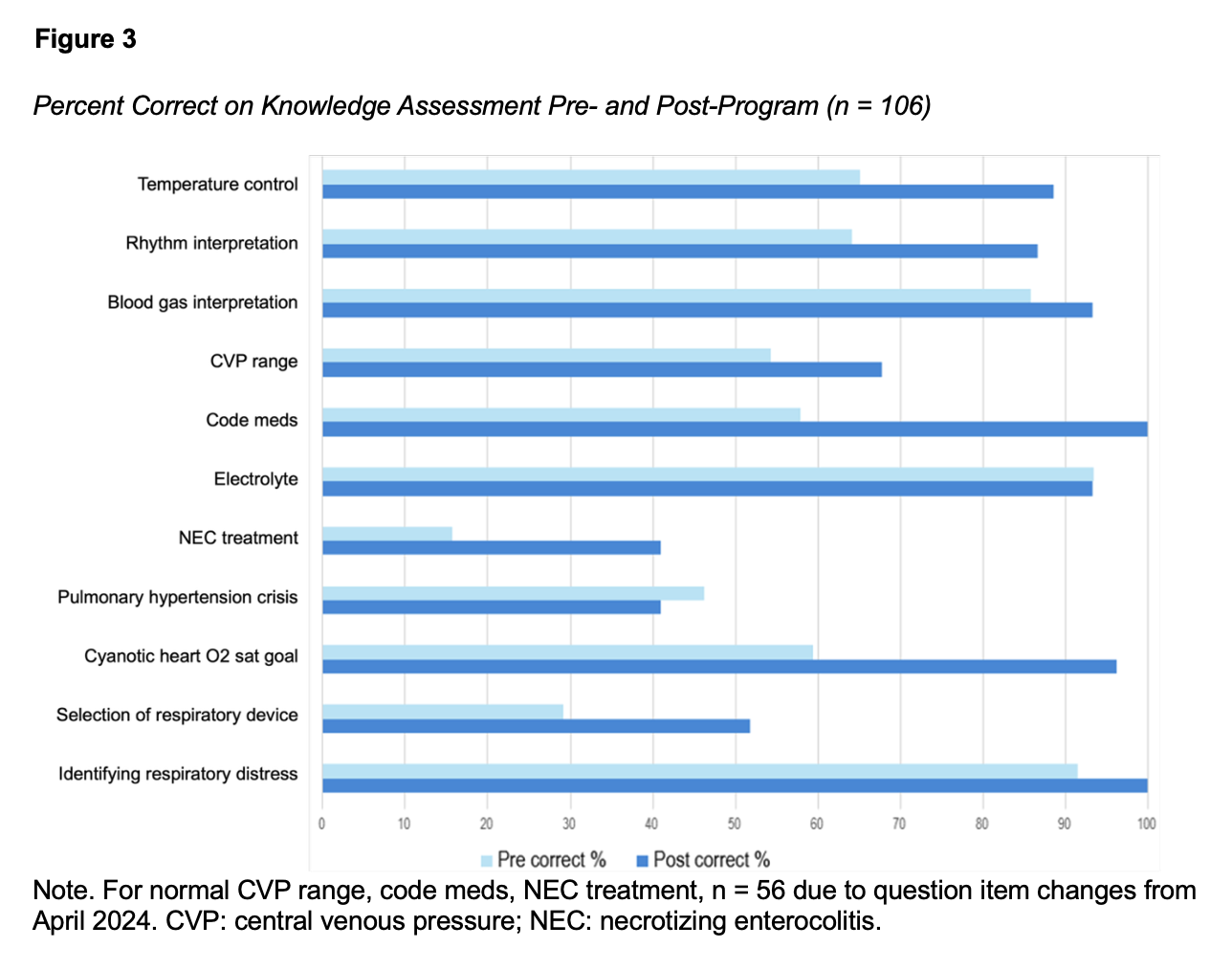
Pre- and post-program surveys assessing comfort (Figure 2) and knowledge (Figure 3) were completed by 106 and 105 participants, respectively. Comfort levels improved in all items (Figure 2), with more participants rating themselves as “very comfortable” or “extremely comfortable”. The items that had the largest increases in comfort levels included “recognizing pediatric respiratory distress,” rising from 35% to 79% (p<0.001), and “participating in a Code Blue,” which increased from 7% to 50% (p<0.001). Participant knowledge increased in 9 of the 11 knowledge areas (Figure 3). The largest improvements were noted in “recognition of appropriate respiratory support” (31% vs. 55%, p=0.001), “Code Blue medications” (58% vs. 100%, p<0.001), and “cardiac rhythm (EKG) interpretation” (68% vs. 91%, p<0.001). Despite these improvements, fewer than half of the participants correctly answered questions related to necrotizing enterocolitis and pulmonary hypertension crisis in the post-program test.
Participant Simulation Feedback
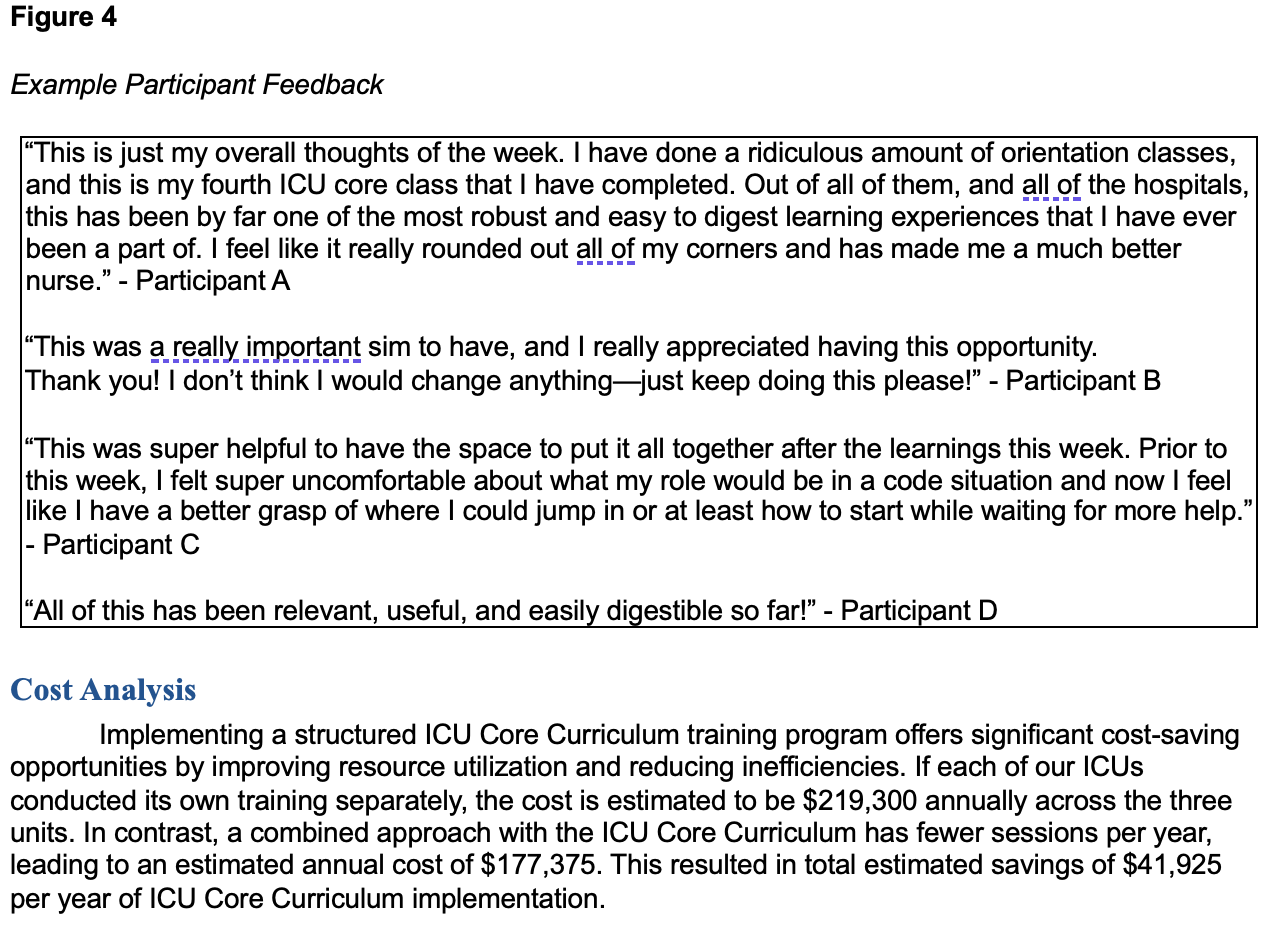
Nurses rated the sessions as highly effective in meeting learning objectives (mean rating 4.8 out of 5, SD=0.5), improving teamwork and communication (4.8, 0.5), and enhancing clinical skills (4.7, 0.5). Participants overwhelmingly felt the simulations provided a psychologically safe learning environment (4.8, 0.4) and that the facilitator enhanced learning (4.8, 0.4). The debriefing was perceived as extremely valuable (4.8, 0.5). Notably, nurses reported a strong likelihood of changing their clinical practice because of the simulations (4.7, 0.5). Survey comments highlighted strong appreciation for the comprehensive and practical nature of simulation exercises (Figure 4).
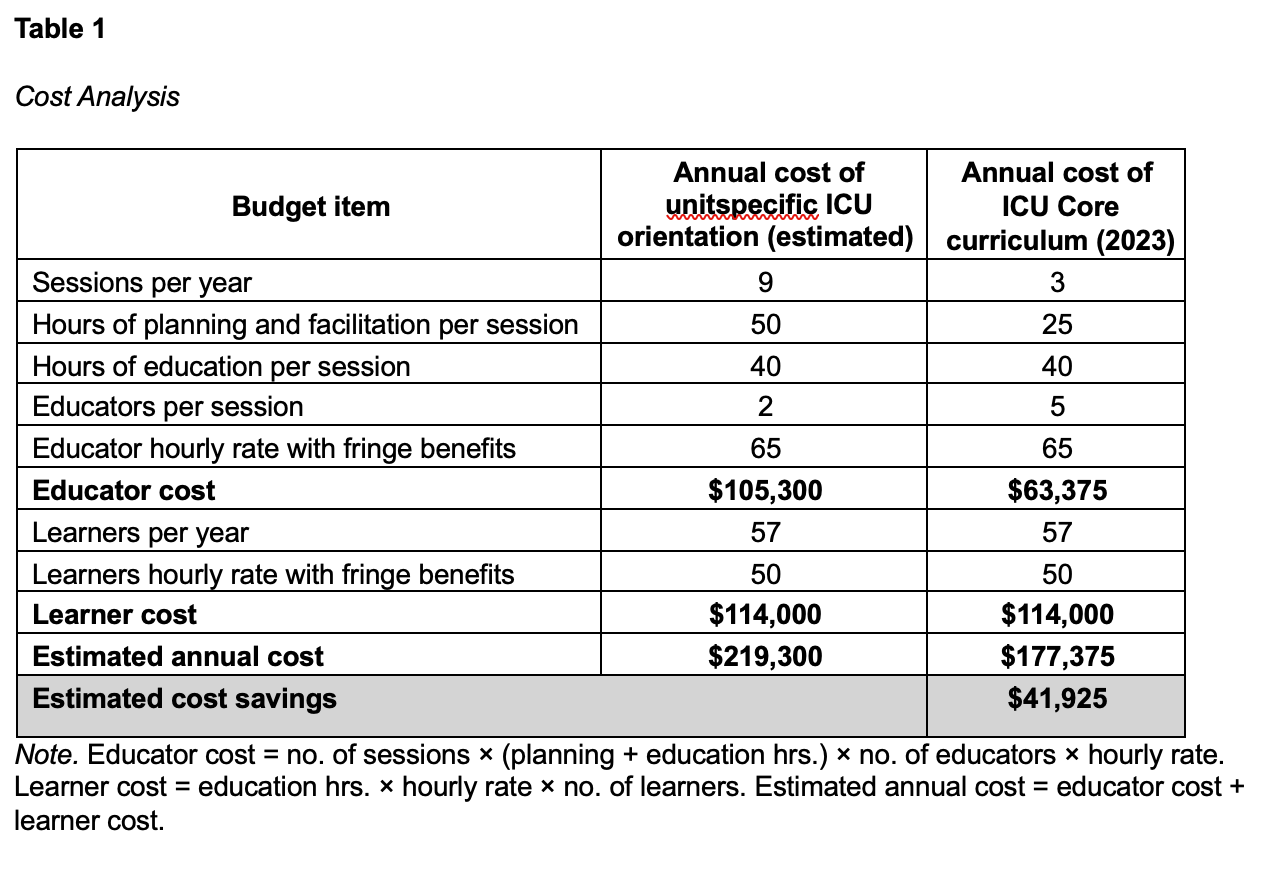
Cost Analysis
Implementing a structured ICU Core Curriculum training program offers significant cost-saving opportunities by improving resource utilization and reducing inefficiencies. If each of our ICUs conducted its own training separately, the cost is estimated to be $219,300 annually across the three units. In contrast, a combined approach with the ICU Core Curriculum has fewer sessions per year, leading to an estimated annual cost of $177,375. This resulted in total estimated savings of $41,925 per year of ICU Core Curriculum implementation.
DISCUSSION
The implementation of the ICU Core Curriculum has shown early promise in addressing the experience-complexity gap and improving the transition of new ICU nurses into high-acuity clinical environments. Through standardization, simulation-based learning, and alignment with evidencebased educational frameworks, this program increased learner comfort and promoted consistent clinical expectations across ICUs. The observed improvements align with existing literature emphasizing simulation’s effectiveness for novice nurses transitioning into practice (RutherfordHemming et al., 2022; Campbell et al., 2022). Our results are similar to those of quasi-experimental ICU simulation studies showing improvement in patient safety knowledge and communication among new ICU nurses (Jung et al., 2023). These results also align with pediatric ICU work demonstrating improved knowledge, teamwork, and confidence via deliberate practice (Karageorge et al., 2020). The ICU Core Curriculum extends this by delivering a weeklong, CHSE/DASH-evaluated onboarding across three PICUs.
Survey and test results demonstrate that the ICU Core Curriculum effectively increased both participants’ comfort and knowledge in managing multiple critical care scenarios. The greatest improvements in participant comfort were seen in using push-pull for fluid administration, Code Blue participation, knowledge of Code Blue medications, and oxygen saturation goal for children with cyanotic congenital heart disease. Persistent discomfort caring for patients with congenital or acquired heart disease, together with low knowledge-assessment scores on the treatment of necrotizing enterocolitis and pulmonary hypertension crisis, highlights areas for future curriculum improvement.
By streamlining educator hours, leveraging shared simulation resources, and consolidating sessions, we estimate that the ICU Core Curriculum is saving our organization more than $40,000 per year. This estimate does not account for the long-term operational savings that could result from strengthening internal training capabilities and reducing reliance on external education resources, such as vendor-led courses, outsourced simulation programs, and third-party continuing education providers. By leveraging the Simulation Center’s resources and expertise, the ICU Core Curriculum ensures consistent, high-quality learning experiences.
Integrating simulation into early clinical training not only fosters knowledge acquisition and enhances clinical confidence but also reduces preceptor workload and promotes a uniform standard of care across the institution’s ICUs. This partnership highlights the Simulation Center’s vital role in advancing clinical education, patient safety, and professional development throughout the organization. Looking ahead, our priorities include long-term follow-up to evaluate knowledge retention and sustained practice change, introducing behavior-based competency checks, and exploring associations with nurse retention and patient outcomes.
Operational Considerations
A key contributor to the success and sustainability of the ICU Core Curriculum was the collaborative partnership between the institutions’ ICU nursing educators and the SSH-accredited Simulation Center. ICU educators led the development, implementation, and ongoing refinement of the curriculum, including educational content design, learner coordination, supply standardization, scheduling workflows, and continuous quality improvement efforts. Simulation educators and CHSOScertified simulation technicians supported the curriculum through consultation on simulation design, management of simulation equipment and environments, audiovisual support, and facilitation of simulation-based learning experiences. During the initial implementation phase, the curriculum required substantial collaboration and operational support from both educator and simulation teams to establish workflows, develop simulation experiences, and standardize delivery across ICUs. As the program matured, many operational processes became more streamlined and sustainable, allowing simulation involvement to transition to a more focused support and consultation role while ICU educators continued to lead ongoing curricular refinement and routine operational management.
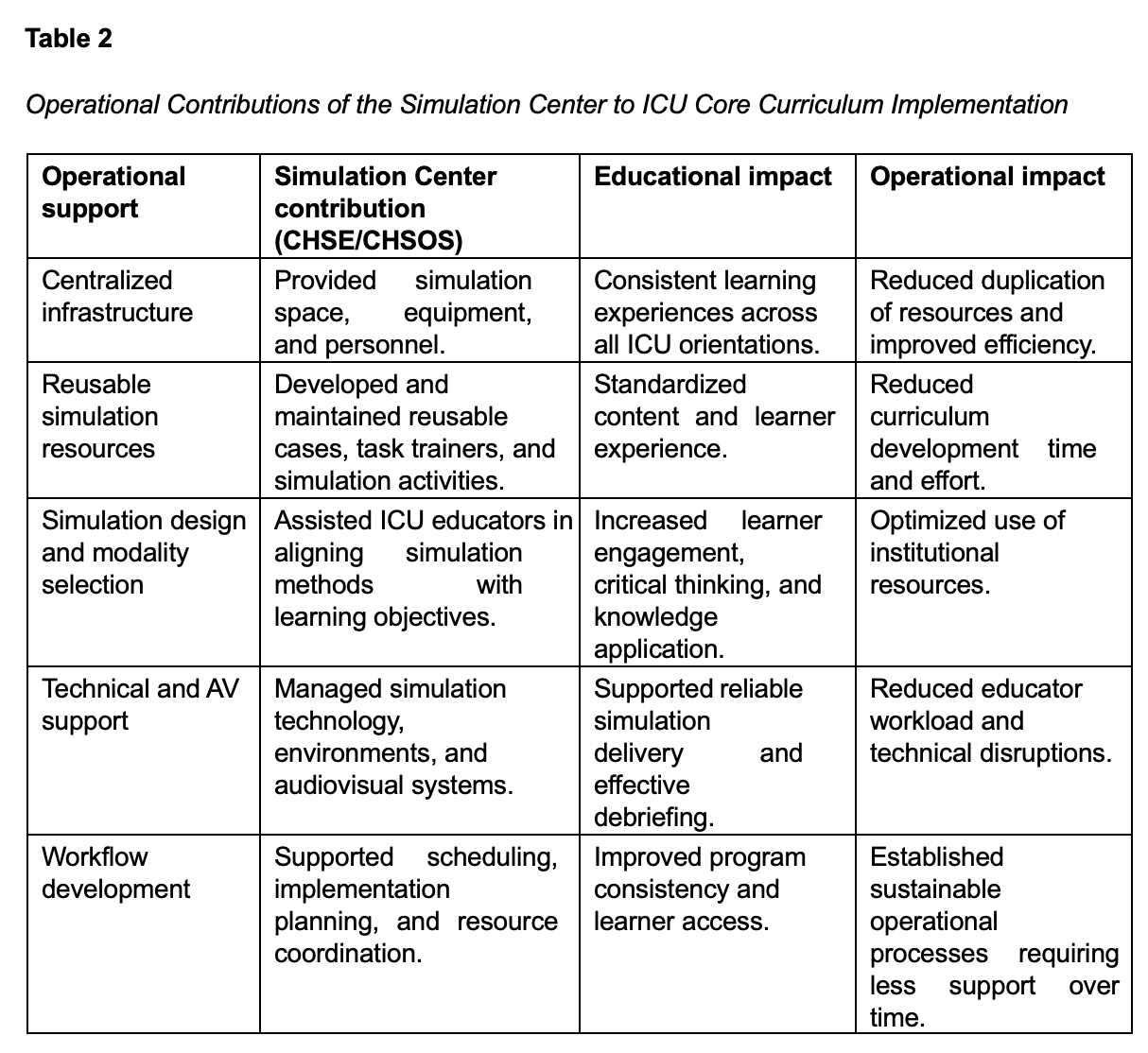
Centralizing portions of the curriculum within the Simulation Center created operational efficiencies by leveraging existing simulation infrastructure, reusable cases, task trainers, and highfidelity simulation resources while promoting consistency across ICU orientation experiences. The integration of multiple simulation modalities, including task trainers, escape rooms, standardized patients, and high-fidelity simulation, allowed the team to align educational objectives with available institutional resources in a cost-effective manner (Boling & Hardin-Pierce, 2016). This evolution in operational support may help organizations considering similar initiatives recognize that, while simulation-based onboarding programs may require significant upfront collaboration and infrastructure development, the ongoing operational demands can become more manageable once workflows, resources, and educational processes are established (Table 2).
Limitations
The following limitations direct our current efforts to further develop and refine the ICU Core Curriculum. Despite intentional scaffolding and progressive escalation of scenario complexity to balance cognitive load, the intensity of a weeklong curriculum may still contribute to cognitive overload and learner fatigue. Participants have indicated in open-text survey feedback that while the training days can be long, they appreciate the opportunity to build on their new knowledge over the course of the week, particularly highlighting the usefulness of bringing everything together during Integration Day. We continue to iteratively adjust and improve the program based on learner feedback to support engagement and knowledge retention.
Although the curriculum incorporates a wide range of simulation modalities, current evaluation efforts have focused primarily on short-term knowledge gains and self-reported comfort. Due to time and resource limitations, individualized assessment of hands-on clinical competencies is currently limited. It remains unclear whether the short-term gains noted immediately following ICU Core translate into long-term knowledge retention or sustained behavior change in clinical practice, or if this improved orientation process is associated with enhanced nurse job satisfaction or nurse retention.
As the program evolved, operational workflows continued to be refined through ongoing collaboration between ICU educators and simulation personnel. Although standardized external training programs, such as the Society of Critical Care Medicine’s Fundamentals of Critical Care Support–Pediatrics (FCCS-P) course (2026), provide structured pediatric critical care education, they may not offer the flexibility needed to tailor content, workflows, equipment, and clinical scenarios to institution-specific patient populations and operational practices. Our institution previously utilized FCCS-P as an adjunct within the Graduate Medical Education Residency Program but transitioned to an internally developed curriculum based on learner feedback and the need for a more customized educational approach. Additionally, scalability remains an operational limitation, as delivery of the ICU Core Curriculum requires substantial educator coordination and sustained faculty involvement throughout the weeklong program. Future efforts should explore hybrid educational models incorporating online modules, asynchronous learning, and in-person simulation training to improve scalability while maintaining educational quality, learner engagement, and operational sustainability.
Future Directions
Future iterations of the ICU Core Curriculum should incorporate structured competency checklists and reassessment of key procedural skills (Lim & Song, 2024). To evaluate the long-term effects of the ICU Core Curriculum, we plan to survey participants three months post-training to assess knowledge retention and comfort levels, as well as explore the association between ICU Core participation and new nurse retention at our institution. Future evaluation efforts should include measures of ICU preceptor satisfaction to determine if standardized ICU onboarding reduces preceptor burden.
Although ICU Core was designed to promote safe, consistent bedside practice, this evaluation did not examine patient-level outcomes. Future work should assess whether standardized ICU onboarding is associated with improved clinical outcomes, such as a reduction in unplanned extubation rates, peripheral intravenous line complications, or device-related pressure injuries, and improvements in patient and family satisfaction.
Future operational efforts should evaluate hybrid delivery models incorporating asynchronous pre-learning, virtual simulation, and distributed facilitation strategies to improve scalability and reduce faculty burden. Additional work is needed to identify operational benchmarks for simulation-based onboarding programs, including educator staffing models, simulation technician utilization, equipment lifecycle management, and return-on-investment metrics. Multi-site implementation studies may further clarify how simulation operations infrastructure influences sustainability and reproducibility across institutions with varying resource availability. Addressing these issues will refine the curriculum and ensure that it continues to meet the evolving needs of an increasingly complex patient population as well as new graduate nurses in both the acute and critical care settings.
CONCLUSION
The ICU Core Curriculum demonstrates the potential for a simulation-enhanced, theory-based onboarding program to improve new ICU nurse readiness in a complex healthcare environment. Standardized simulation experiences increased learner knowledge and confidence, with the potential to reduce preceptor burden and promote consistency across ICU units. By consolidating orientations, this program generated an estimated cost savings of $41,925 annually. Guided by scaffolded learning, INACSL standards, and CHSE/CHSOS-facilitated simulation in an SSH-accredited center, this model shows strong potential for expansion to other nursing specialties.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Please cite this article as: Camacho, C., Brophy, A., Valido, L., Tanda, R., Tucker, A., Heater, T., & Kalvas, L. B. (2026). Revolutionizing new hire education in critical care: The power and cost-savings of multimodal simulation. Simulation Technology & Operations Resource Magazine, 5(2), 44-56. ISSN: 3070-3506.
REFERENCES
American Association of Critical-Care Nurses. (2022). AACN’s Competence Framework for Progressive and Critical Care: Initial Competency 2022. American Association of Critical- Care Nurses. ISBN: 9781929209026.
Al-Khayat T., Carter S., Mauger M., Patel A., Patel K., Chavarria L. (2024). Implementing the Debriefing Assessment for Simulation in Healthcare (DASH) Tool for training medical faculty. Cureus, 16(9), e69290. https://doi.org/10.7759/cureus.69290
Bloom, B. S. (1956). Taxonomy of Educational Objectives, Handbook I: The Cognitive Domain. New York: David McKay Co Inc. ISBN: 0582280109.
Boling, B. & Hardin-Pierce, M. (2016). The effect of high-fidelity simulation on knowledge and confidence in critical care training: An integrative review. Nurse Education in Practice,16(1), 287-293. https://doi.org/10.1016/j.nepr.2015.10.004
Campbell, A., Ascenzi, J., & Busch, D. (2022). An integrative review regarding knowledge and self-competency of pediatric and neonatal critical care transport nurses. Air Medical Journal, 41(5), 484–490. https://doi.org/10.1016/j.amj.2022.06.006
Gamble, M. (2026, April 22). The cost of nurse turnover in 10 points | 2026. Becker’s Hospital Review. https://www.beckershospitalreview.com/workforce/the-cost-of- nurse-turnover-in-10points-2026/
INACSL Standards Committee, Watts, P.I., McDermott, D.S., Alinier, G., Charnetski, M., & Nawathe, P.A. (2021a). Healthcare Simulation Standards of Best Practice™ Simulation
Design. Clinical Simulation in Nursing, 58, 14-21. https://doi.org/10.1016/j.ecns.2021.08.009
INACSL Standards Committee, Miller, C., Deckers, C., Jones, M., Wells-Beede, E., & McGee, E. (2021b). Healthcare Simulation Standards of Best Practice™ Outcomes and Objectives.
Clinical Simulation in Nursing, 58, 40-44. https://doi.org/10.1016/j.ecns.2021.08.013
Jones, C. B. (2021). The cost of nurse turnover: Part 2—Application of the nursing turnover Cost calculation methodology. Journal of Nursing Administration, 51(3), 123–129. https://doi.org/10.1097/NNA.0000000000000995
Jung, S. J., Song, J. -E., Bae, S. H., Lee, Y., Gwon, S. H., Park, J. H. (2023). Simulation-based training program on patient safety management: A quasi-experimental study among new intensive care unit nurses. Nurse Education Today, 126, 105823. https://doi.org/10.1016/j.nedt.2023.105823
Karageorge, N., Muchler, V., Toper, M., Hueckel, R. (2020). Using simulation with deliberate practice to improve pediatric ICU Nurses’ knowledge, clinical teamwork, and confidence. Journal of Pediatric Nursing, 54, 58-62. https://doi.org/10.1016/j.pedn.2020.05.020
Lim, C. Y., & Song, M.R. (2024). Sustained effect of simulation-based resuscitation education on knowledge, self-confidence and performance ability of neonatal intensive care unit nurses. Journal of Continuing Education in Nursing, 55(2), 79-86. https://doi.org/10.3928/00220124-20231109-05
Masso, M., Sim, J., Halcomb, E., Thompson, C. (2022). Practice readiness of new graduate nurses and factors influencing practice readiness: A scoping review of reviews.
International Journal of Nursing Studies, 129, 104208. https://doi.org/10.1016/j.ijnurstu.2022.104208
Palmer, B., Valido, L.,Tucker, A.,Tanda, R., Opperman, C. (2025). Collaborative Core Curriculum Initiative: Alignment with nursing professional development roles. Journal for Nurses in
Professional Development, 41(2), 85-90, https://doi.org/10.1097/NND.0000000000001115
Rutherford-Hemming T, Herrington A, Newsome L. (2022). The use of simulation-based education with new graduate nurses in emergency department and acute care settings:
A scoping review. Journal of Continuing Education in Nursing, 53(7), 301-306. https://doi.org/10.3928/00220124-20220603-05
Schwengel, D., Villagrán, I., Miller, G., Miranda, C., & Toy, S. (2025). Multimodal assessment in
clinical simulations: A guide for moving towards precision education. Medical Science Educator, 35, 1025–1034. https://doi.org/10.1007/s40670-024-02221-7
Society of Critical Care Medicine. Fundamentals of Critical Care Support: Pediatrics (FCCS-P). Accessed May 6, 2026. https://sccm.org/education-center/educational programming/fundamentals/pediatric-fundamental-critical-care-support
Zann, A., Harwayne-Gidansky, I., & Maa, T. (2021). Incorporating simulation into your Plan-Do- Study-Act Cycle. Pediatric annals, 50(1), e25–e31. https://doi.org/10.3928/19382359-20201213-01