AUTHORS
Hanh M. T. Nguyen, MD, MHPE1; Hoa T. T. Doan, MD, MHPE1; Bao Q. Le, MD1; Anh T. Pham, MD1; Loi N. Ho, MD1; Ngan K. Tran, MEd1; Ni H. T. Huynh, BS1; Ly T. T. Ngo, BS1; Thanh M. N. Bui, MD1 ; Hoang M. Dinh, BS1
1Center for Advanced Training in Clinical Simulation, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam
Corresponding Author
Hanh M. T. Nguyen, nguyenthimyhanh@ump.edu.vn
SUMMARY
Achieving international simulation accreditation in low- and middle-income countries presents persistent operational challenges, including limited infrastructure, financial constraints, and workforce capacity gaps. While the Society for Simulation in Healthcare (SSH) provides comprehensive accreditation standards, practical guidance on implementing them in resourcelimited settings remains scarce. This article presents a practical implementation roadmap describing how the Center for Advanced Training in Clinical Simulation (ATCS) in Vietnam operationalized SSH standards over a seven-year period. Specifically, we describe how policies were developed, procedures were standardized, and a continuous quality improvement (CQI) framework was established and iteratively refined to align with accreditation requirements. We further detail the operational processes, governance structures, documentation systems, and internal review mechanisms that supported progression toward full SSH accreditation, with an emphasis on how these components were adapted to local constraints. Practical lessons and a replicable, step-by-step implementation roadmap are provided to support simulation centers pursuing accreditation in similar resource-limited contexts.
INTRODUCTION
Patient safety remains a global priority, particularly in low- and middle-income countries, where resource constraints often limit access to standardized training environments (WHO, 2021; WHO, 2023; Kruk et al., 2018). Simulation-based education (SBE) offers a structured and safe platform for improving clinical competence and reducing preventable harm (Issenberg et al., 2005; McGaghie et al., 2011). However, sustaining high-quality simulation programs requires more than instructional innovation; it demands strong governance, standardized procedures, and ongoing quality oversight.
The Society for Simulation in Healthcare (SSH) accreditation standards provide a comprehensive framework for simulation program quality (SSH, 2021). While these standards are widely recognized, practical guidance on how to operationalize them in resource-limited settings remains limited. Beginning in 2017, the Center for Advanced Training in Clinical Simulation (ATCS) at the University of Medicine and Pharmacy at Ho Chi Minh City (UMP) undertook a phased institutional strategy to align operations with SSH standards. Over seven years, ATCS developed structured policies, standardized procedures, documentation systems, and a continuous quality improvement (CQI) process to support sustainable accreditation readiness. This article describes the operational processes, governance structures, policy development, and internal review mechanisms used to implement SSH standards in a resource-limited context. Practical lessons and replicable strategies are shared to support other simulation centers pursuing accreditation. This paper aims to provide a practical, step-by-step implementation roadmap to support simulation centers in aligning with SSH accreditation standards in resource-limited settings.
INSTITUTIONAL CONTEXT AND EDUCATIONAL SETTING
Establishment of the ATCS took place during a university-wide transition toward competencybased medical education (CBME) at the UMP, beginning in 2016-2017. The CBME reform emphasized integrated learning, professionalism, interprofessional education, and competency-based assessment aligned with national healthcare priorities. SBE was identified as a core strategy to standardize skills training and ensure safe clinical practice. ATCS was founded to support the university’s educational mission by enhancing the quality of clinical skills training and competency assessment, while advancing medical education research to improve patient safety and healthcare quality in Vietnam and the Southeast Asia region. The center’s development was guided by international evidence demonstrating that SBE improves learning outcomes, promotes interprofessional collaboration, and facilitates the transfer of clinical skills into real-world practice.
In 2017, UMP established a formal collaboration with Texas Tech University Health Sciences Center at El Paso (TTUHSC El Paso) to strengthen faculty capacity and provide technical consultation for the development and operation of the simulation center. This partnership delivered structured faculty development programs, guidance on simulation pedagogy and assessment, as well as consultation on operational management and governance, thereby supporting the establishment of ATCS as a dedicated simulation center.
INTERVENTION DESCRIPTION Strategic Intervention: Phased Development of a Simulation Center
The implementation roadmap consists of four key operational components: (1) governance structure, (2) instructional design standardization, (3) assessment and quality assurance, and (4) continuous quality improvement systems. The central initiative involved developing an SBE system aligned with SSH accreditation standards over seven years. An initial Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis was conducted through multidisciplinary stakeholder engagement, with faculty, administrators, and technical staff, to systematically evaluate infrastructure, workforce capacity, operational processes, and existing training programs. This analysis ensured that strategic planning was grounded in both institutional realities and accreditation requirements. Findings from the SWOT analysis informed the development of a phased strategic roadmap, in which priorities were sequenced based on feasibility and impact. Leadership support and international collaboration were leveraged as enabling factors, while gaps, such as variability in faculty competency, resource limitations, and increasing learner demand were addressed in each phase.
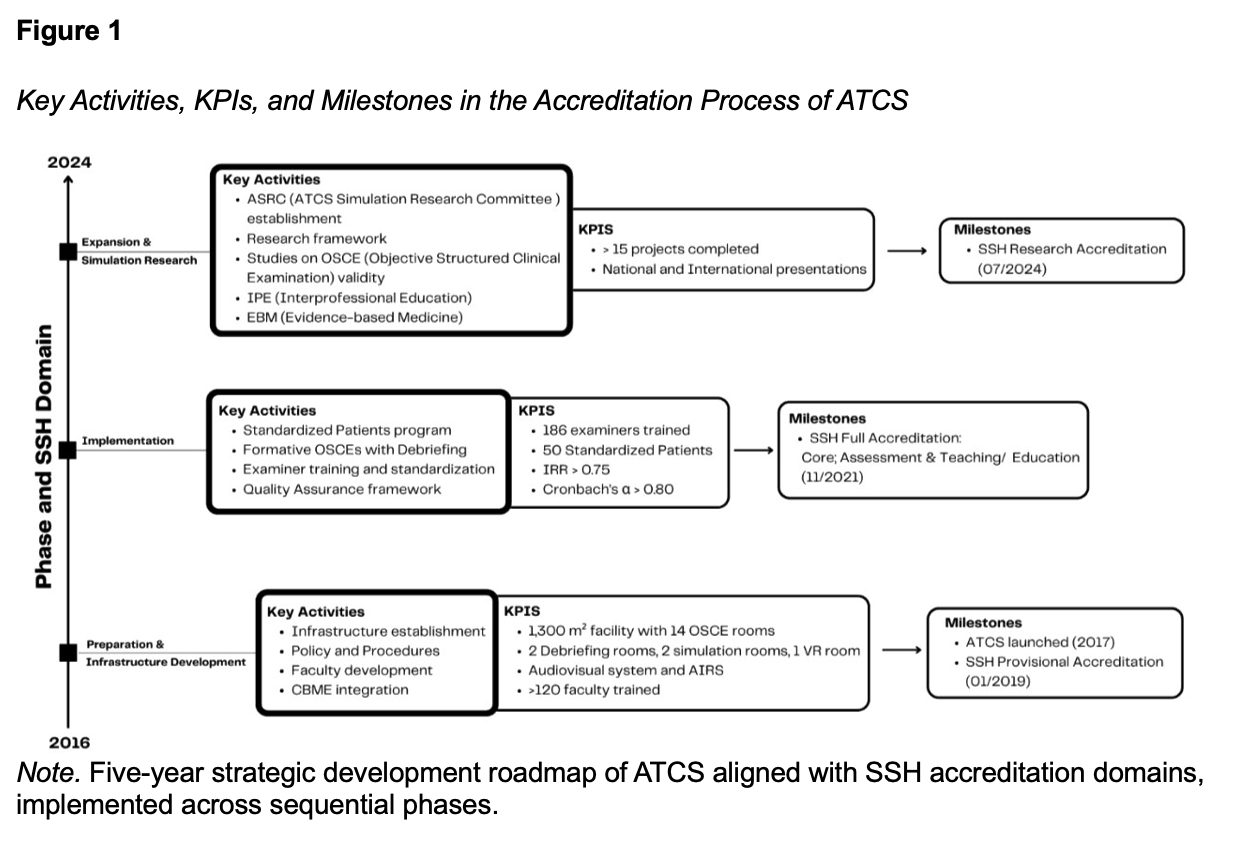
To operationalize this roadmap within a resource-limited context, ATCS implemented iterative strategic cycles (Figure 1) incorporating predefined key performance indicators (KPIs), milestonebased benchmarks, and embedded CQI processes. KPIs were regularly monitored through internal review meetings and documentation audits, enabling data-driven adjustments to implementation strategies. Each phase was explicitly mapped to specific SSH accreditation domains, with clearly defined activities, measurable outcomes, and structured review mechanisms. This phased operational model was intentionally designed to balance structure and flexibility, allowing incremental alignment with international standards while adapting to evolving institutional capacity and resource constraints.
IMPLEMENTATION PROCESSES Governance Structure to Support Simulation Operations
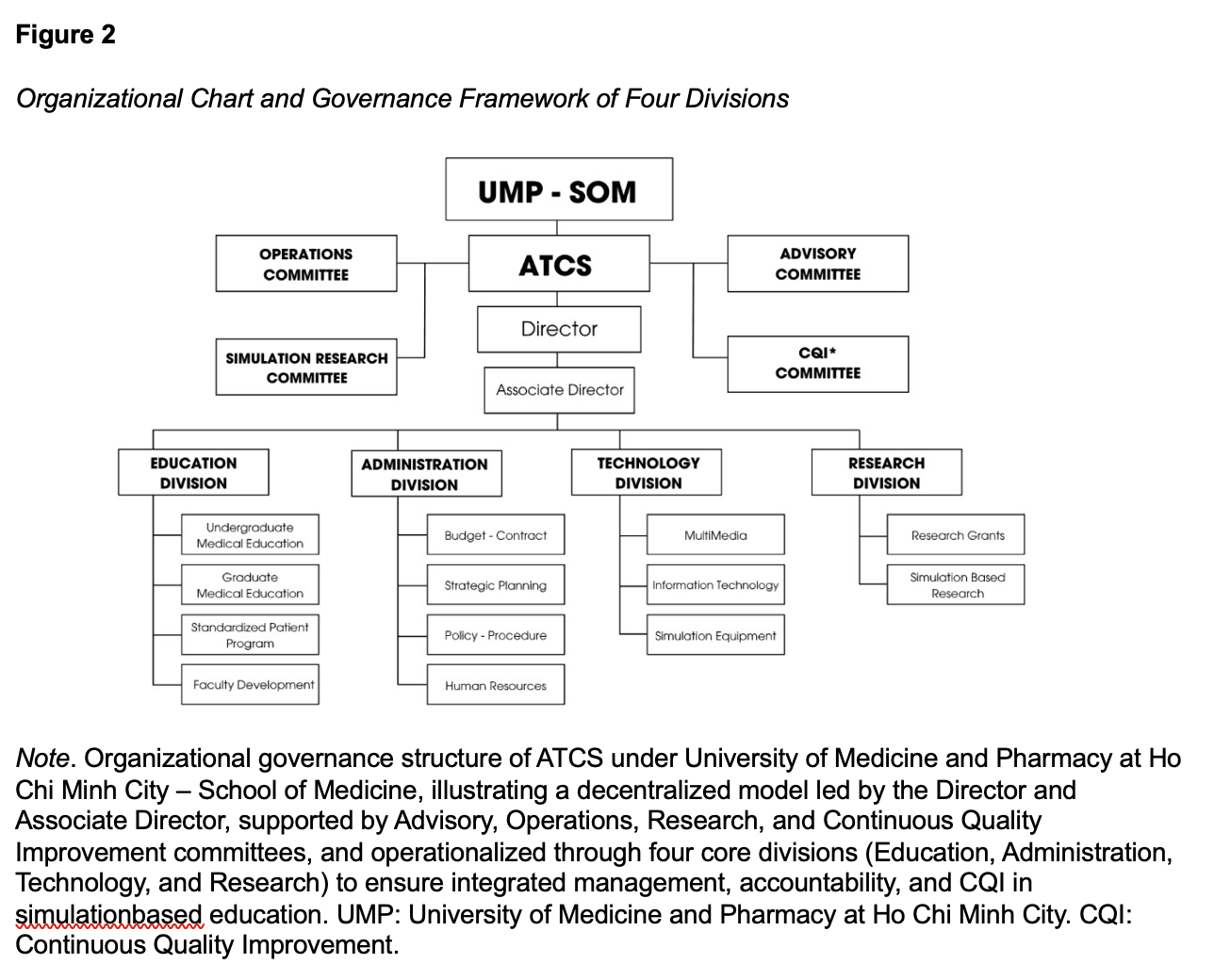
As ATCS expanded its scope and complexity, a decentralized governance structure was implemented to ensure operational consistency, accountability, and sustainable growth (Figure 2). Rather than centralizing decision-making within a single leadership role, responsibilities were distributed across committees and operational divisions with clearly defined reporting lines. All operational activities are guided by formal policies, standard operating procedures, and written role descriptions. These documents serve as the foundation for onboarding, quality assurance, and operational continuity. Four standing committees support governance:
- The Advisory Committee provides strategic oversight and reviews program performance.
The Operations Committee coordinates daily scheduling, workflow management, and resource allocation.
The ATCS Simulation Research Committee ensures ethical oversight and research integrity.
The CQI Committee applies Plan–Do–Study–Act (PDSA) cycles to evaluate performance metrics and drive process improvements.
Operational responsibilities are implemented through four core divisions: Education, Administration, Technology, and Research. Each division maintains defined deliverables while functioning within an integrated reporting framework led by the Director and Associate Director. This governance model allows simulation operations to scale while maintaining quality control, research compliance, and operational transparency. Embedding CQI processes into routine workflow has strengthened sustainability and improved responsiveness to stakeholder needs.
INSTRUCTIONAL DESIGN OF SIMULATION ACTIVITIES
As part of the implementation roadmap, ATCS implemented a standardized instructional design workflow to ensure consistency and quality across programs for all simulation activities. This approach was adopted to reduce variability in teaching practices and to ensure alignment with CBME outcomes and national healthcare priorities, while maintaining flexibility across disciplines and learner levels.
Learning objectives are developed through a structured gap analysis process that integrates multiple data sources, including learner performance data, faculty feedback, and observed deficiencies in clinical practice. This is complemented by stakeholder consultation to ensure relevance to both educational and clinical needs. Proposed activities then undergo a multidisciplinary review involving curriculum committees, assessment units, quality assurance teams, and simulation operations staff, ensuring both educational rigor and operational feasibility prior to institutional approval. All simulation activities follow a defined seven-step development pathway designed to ensure systematic alignment between objectives, instructional strategies, and assessment:
- Conduct gap analysis to identify priority learning needs.
Develop SMART learning objectives (Chatterjee & Corral, 2017) to ensure clarity in expected learning outcomes and to enable objective assessment of learner performance. SMART
learning objectives are defined as Specific, Measurable, Achievable, Relevant, and Timebound.
- Map objectives to program outcomes to maintain curricular alignment.
- Select appropriate instructional strategies based on learning goals and context.
- Develop scenario scripts and facilitator guides to standardize delivery.
- Determine simulation modality and fidelity level based on resource availability and educational value.
Implement sessions with structured pre-briefing and debriefing using the Promoting Excellence and Reflective Learning in Simulation (PEARLS) framework (Eppich & Cheng, 2015) to optimize learning outcomes.
Standardized templates, scenario development checklists, and facilitator guides are maintained in a shared digital repository with version control. This system supports consistency, facilitates iterative updates, and enables efficient scaling of simulation activities across programs.
SIMULATION MODALITY AND FIDELITY
Within this implementation roadmap, ATCS applies a practical decision-making principle of “right modality, right objective, right learner” (Carey & Rossler, 2025) to guide the selection of simulation methods. This approach ensures alignment between learning goals, learner level, and available resources while maintaining cost-effectiveness.
Standardized patients (SPs) serve as the primary modality for communication skills, professionalism, and clinical reasoning training. Task trainers and low-to-mid fidelity simulators are used for procedural skill development when psychomotor performance is the primary objective. Highfidelity mannequins and virtual simulation are reserved for advanced learners and complex clinical scenarios requiring team coordination, crisis management, or integrated clinical decision-making.
Modality selection is determined during the instructional design phase using a structured planning checklist. This checklist incorporates key domains, including learning objectives, learner readiness, faculty availability, equipment requirements, and operational feasibility, as illustrated in Figure 3.
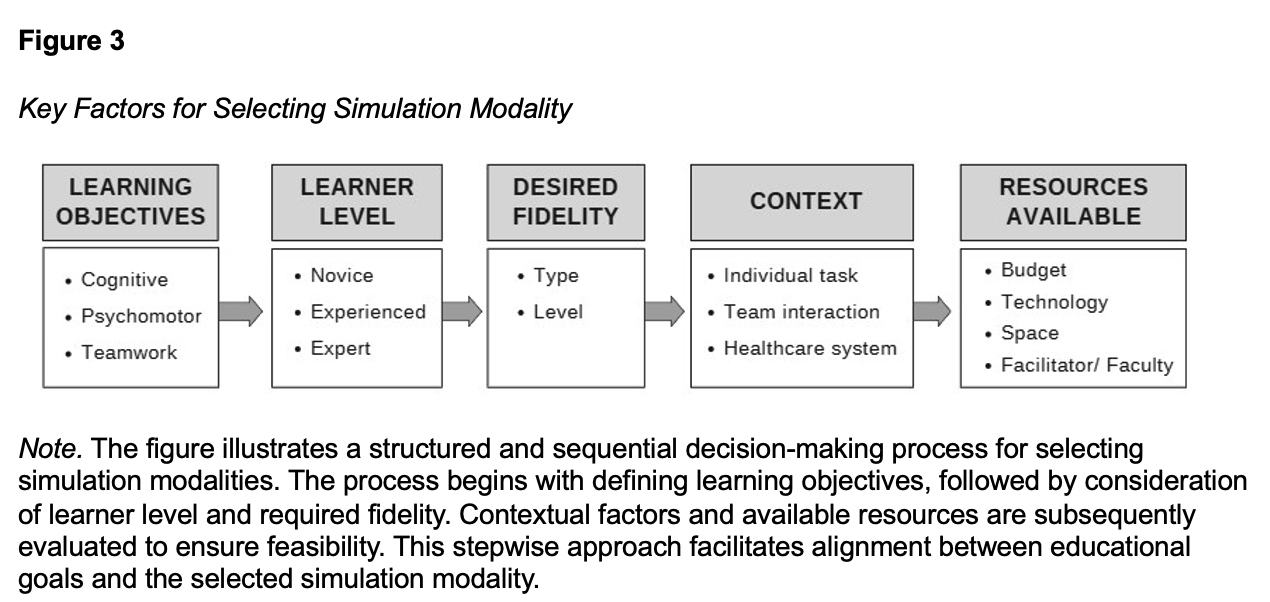
By prioritizing educational outcomes over technology-driven implementation, ATCS ensures efficient resource utilization - an approach particularly relevant for simulation centers operating in resource-limited settings.
LEARNER ORIENTATION AND PSYCHOLOGICAL SAFETY
All simulation sessions begin with a structured orientation and pre-briefing to establish expectations, clarify learning objectives, and reinforce principles of psychological safety. Standardized ground rules are reviewed at the beginning of each session, emphasizing confidentiality, mutual respect, and a non-judgmental learning environment.
Facilitators explicitly normalize errors as a natural part of the learning process and encourage learners to engage openly in discussion and reflection. During debriefing, faculty apply the PEARLS framework to guide structured reflection, explore learners’ clinical reasoning, and maintain a supportive and constructive tone aimed at helping students develop actionable plans to improve their clinical performance. To ensure consistency, orientation scripts and debriefing prompts are embedded within facilitator guides. This standardized approach reduces performance anxiety, promotes honest participation, and strengthens learner engagement across programs.
By integrating psychological safety into routine operational practice rather than treating it as a theoretical concept, ATCS fosters a safe and effective learning environment while maintaining structured educational rigor.
FACULTY AND STAFF DEVELOPMENT
Faculty and staff development are integrated into ATCS operational systems to ensure instructional quality and long-term sustainability. Since 2017, core faculty have participated in structured training in simulation center operations and SBE through a memorandum of understanding with TTUHSC El Paso.
This collaboration was operationalized through the Collaborative Educational Program, a longitudinal faculty development program comprising core modules in competency-based medical education, teaching and assessment, medical education research (including Objective Structured Clinical Examination (OSCE) and standardized patient methodologies), simulation-based clinical training, and leadership development. Training was delivered through a combination of on-site workshops, hands-on simulation sessions, and longitudinal mentorship across multiple cohorts. By 2022, more than 220 faculty members had participated in these collaborative programs, contributing to institutional capacity building and supporting the standardization of simulation-based education practices. Selected faculty also completed short-term intensive training at the simulation center in El Paso, focusing on OSCE implementation, simulation technologies, and standardized patient programs. These activities collectively strengthened local expertise and contributed to institutional readiness for SSH accreditation.
In addition, ATCS conducts regular internal development sessions focusing on simulation equipment management, scenario facilitation, and structured onboarding for new staff. Faculty are encouraged to engage in simulation-related scholarship to support academic integration. In parallel, in-house workshops organized by the Faculty Development Unit address SBE, OSCE implementation, standard-setting methodologies, and active learning design.
To ensure operational consistency, ATCS maintains a centralized faculty database that tracks expertise, training history, teaching experience, and learner feedback. Faculty assignments are aligned with documented competencies. A structured mentorship model pairs junior faculty with experienced mentors to strengthen facilitation skills, standardize instructional quality, and support ongoing professional development.
TEACHING, ASSESSMENT, AND QUALITY ASSURANCE
Teaching quality and assessment at ATCS are supported by a structured faculty qualification and quality assurance system designed to ensure consistency, reliability, and alignment with accreditation standards. Faculty members are required to complete formal professional development in SBE prior to serving as instructors or examiners, ensuring a standardized baseline of teaching and assessment competency.
Between 2018 and 2021, more than 186 faculty members underwent structured assessment training focused on key principles, including fairness, reliability, feasibility, confidentiality, and psychological safety. This training included calibration exercises and performance benchmarking to ensure consistent scoring practices. Examiners were selected based on both clinical expertise and assessment competence, only receiving formal assignment after achieving acceptable levels of scoring agreement during calibration.
To support continuous quality improvement, ATCS implemented a multi-source evaluation system using standardized tools to assess learners, instructors, and standardized patients (SPs). A routine 360° feedback process was conducted to systematically collect input from learners, peers, SPs, and operational staff. This approach was designed to provide comprehensive insights into instructional effectiveness and to identify areas for targeted improvement.
The OSCE serves as the primary competency-based assessment format. OSCEs are developed using blueprint-driven design to ensure alignment with CBME outcomes and national healthcare priorities. Quality assurance measures include pre-exam calibration sessions, pilot testing of stations, standardized scenarios and checklists, electronic scoring systems, and structured postexam reviews. Assessment data are systematically analyzed to support CQI initiatives. Video monitoring, examiner debriefings, and targeted recalibration workshops are used to identify variability in scoring and improve inter-rater reliability. In addition, formative OSCE sessions incorporate structured debriefing and video-assisted review to enhance reflective learning and better prepare learners for high-stakes assessments and clinical practice.
RESEARCH
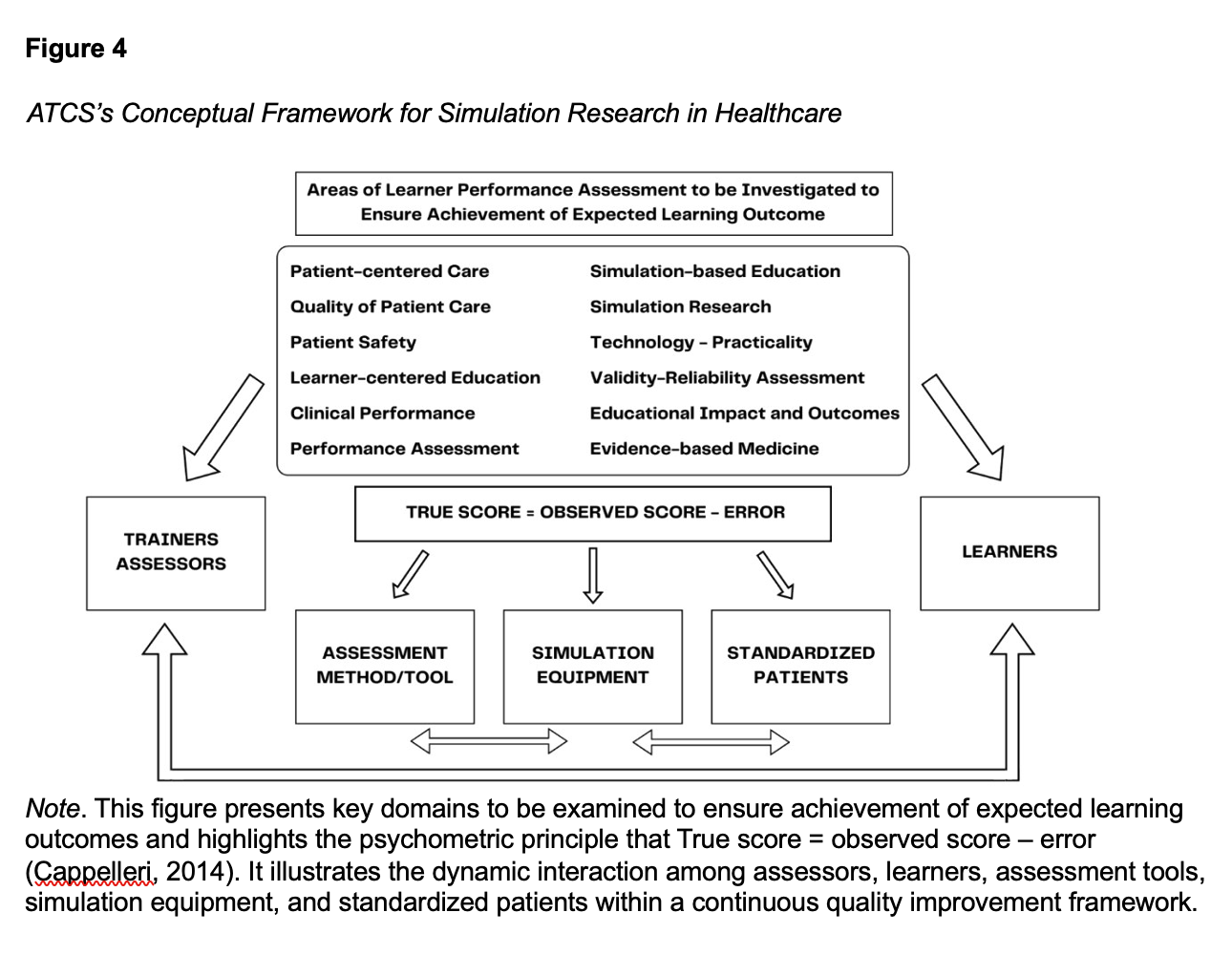
In alignment with ATCS’s mission, ATCS established a Simulation Research Framework (Figure 4) to support study oversight, monitor assessment processes, and identify potential sources of variability in competency evaluation (e.g., examiners, assessment tools, equipment, and standardized patients).
Operational guidelines were developed for UMP faculty and staff conducting simulation-based research. These include requirements for protocol review, ethical approval, and internal methodological oversight. Research proposals undergo internal review to ensure alignment with institutional priorities and quality standards before implementation. Research findings are shared through conferences, peer-reviewed publications, and institutional quality improvement meetings. Key insights are incorporated into faculty development activities, assessment recalibration, and program redesign to strengthen operational effectiveness. Moving forward, ATCS will prioritize three applied research domains:
- Strengthening the validity and reliability of assessment tools
- Evaluating the impact of simulation on clinical performance
- Integrating evidence-based medicine and interprofessional collaboration into simulation training
DISCUSSION
The development of ATCS demonstrates that SSH accreditation can be effectively operationalized in resource-limited settings when governance systems, standardized procedures, and CQI are embedded into routine operations. This experience can be conceptualized as a practical implementation roadmap, consisting of phased development, governance structuring, standardized instructional processes, and embedded CQI systems. These elements provide transferable strategies that can be adapted by other simulation centers operating in resource-limited settings. Rather than viewing accreditation as a one-time achievement, ATCS approached it as an operational framework that guides decision-making, documentation standardization, and performance monitoring.
Initial challenges included financial constraints, variability in faculty preparedness, and limited familiarity with accreditation requirements. Instead of prioritizing high-cost technology investments, ATCS first focused on establishing governance structures, clearly defining roles and reporting lines, and standardizing operational processes. This ensured operational continuity during staff transitions and reduced variability in program implementation.
A structured CQI system played a central role. By integrating PDSA cycles into daily workflows, performance indicators were reviewed regularly rather than only during accreditation preparation. This approach enabled small but continuous adjustments in scheduling, scenario design, faculty calibration, and assessment processes. As a result, accreditation readiness became an ongoing operational condition rather than a periodic activity.
Alignment among instructional design, faculty development, and assessment systems strengthened institutional credibility and reliability. Blueprint-driven OSCE implementation, structured examiner calibration processes, and centralized data management ensured consistency and defensibility of assessment outcomes. In resource-limited contexts, these structures are particularly important for balancing efficiency with accountability.
The establishment of a formal partnership with TTUHSC El Paso in 2017 represented a pivotal turning point in our accreditation journey. In contrast to isolated internal efforts, this structured international collaboration enabled a more systematic and guided approach to aligning with SSH standards. Findings from our experience suggest that such partnerships can play a critical role in addressing common barriers in resource-limited settings, particularly in relation to faculty development, standardization of processes, and access to educational resources. A key contribution of this collaboration was the provision of external expertise, which facilitated not only the development but also the critical appraisal of institutional policies and procedures. This external perspective was instrumental in identifying gaps that may not have been apparent through internal review alone, thereby strengthening the overall quality and consistency of implementation. In addition, the iterative nature of mentorship, combined with mock accreditation activities and continuous feedback, supported a cycle of ongoing refinement consistent with the principles of continuous quality improvement.
Furthermore, access to structured training programs, simulation equipment, and digital resources through the partnership significantly enhanced local capacity, allowing for more rapid and effective adoption of competency-based and learner-centered educational approaches. These findings align with previous literature (Robinson et al., 2024) emphasizing the importance of collaborative networks in advancing simulation-based education, particularly in low- and middleincome countries.
Collectively, our experience suggests that strategic international collaboration should not be viewed merely as supplementary support, but rather as a core component of successful accreditation efforts in resource-constrained contexts. Such partnerships offer a scalable and potentially replicable model for other institutions seeking to bridge resource gaps while maintaining alignment with international standards. For simulation operations specialists, this experience highlights the following practical considerations:
- Governance should be established before expanding technology investments.
- Written policies and standardized workflows reduce operational variability.
CQI processes should be embedded into routine operations, not reserved for accreditation cycles.
- Faculty calibration and assessment oversight are essential for maintaining quality.
Documentation and data management systems are foundational for sustainability and scalability.
When operationalized through clear policies, standardized procedures, and continuous monitoring, accreditation can function as a strategic management tool that strengthens simulation systems in resource-limited environments.
CONCLUSION
The seven-year development of ATCS demonstrates that simulation centers in resourcelimited settings can establish and sustain structured simulation programs aligned with international standards through phased planning, strong governance, and sustained faculty development. Beyond accreditation, this process strengthened assessment systems, faculty capability, operational consistency, and a culture of patient safety and continuous quality improvement. The ATCS model offers a practical and transferable implementation roadmap for institutions in low- and middle-income countries seeking to build, scale, and sustain SBE while remaining responsive to local resource constraints.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Please cite this article as: Nguyen, H. M. T., Doan, H. T. T., Le, B. Q., Pham, A. T., Ho, L. N., Tran, N. K., Huynh, N. H. T., Ngo, L. T. T., Bui, T. M. N., & Dinh, H. M. (2026). From scratch to full SSH accreditation: A practical implementation roadmap from a simulation center in Vietnam. Simulation Technology & Operations Resource Magazine, 5(2), 13-23. ISSN: 3070-3506.
REFERENCES
Issenberg, S. B., McGaghie, W. C., Petrusa, E. R., Gordon, D. L., & Scalese, R. J. (2005). Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Medical Teacher, 27(1), 10–28. https://doi.org/10.1080/01421590500046924
Cappelleri, J. C., Lundy, J. J., & Hays, R. D. (2014). Overview of classical test theory and item response theory for the quantitative assessment of items in developing patient-reported outcomes measures. Clinical Therapeutics, 36(5), 648–662. https://doi.org/10.1016/j.clinthera.2014.04.006
Carey, J. M., & Rossler, K. (2025). The how when why of high-fidelity simulation. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK559313/
Chatterjee, D., & Corral, J. (2017). How to write well-defined learning objectives. Journal of Education in Perioperative Medicine, 19(4), E610. https://pubmed.ncbi.nlm.nih.gov/29766034/
Eppich, W., & Cheng, A. (2015). Promoting excellence and reflective learning in simulation (PEARLS): Development and rationale for a blended approach to health care simulation debriefing. Simulation in Healthcare, 10(2), 106–115. https://doi.org/10.1097/SIH.0000000000000072
Kruk, M. E., Gage, A. D., Joseph, N. T., Danaei, G., García-Saisó, S., & Salomon, J. A. (2018). Mortality due to low-quality health systems in the universal health coverage era: A systematic analysis of amenable deaths in 137 countries. The Lancet, 392(10160), 2203–2212. https://doi.org/10.1016/S0140-6736(18)31668-4
McGaghie, W. C., Issenberg, S. B., Cohen, E. R., Barsuk, J. H., & Wayne, D. B. (2011). Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Academic Medicine, 86(6), 706–711. https://doi.org/10.1097/ACM.0b013e318217e119
Robinson, S. J. A., Ritchie, A. M. A., Pacilli, M., Nestel, D., McLeod, E., & Nataraja, R. M. (2024). Simulation-based education of health workers in low- and middle-income countries: A systematic review. Global Health: Science and Practice, 12(6), e2400187. https://doi.org/10.9745/GHSP-D-24-00187
Society for Simulation in Healthcare (SSH). (2021). Full accreditation. https://www.ssih.org/full-accreditation
World Health Organization (WHO). (2021). Global Patient Safety Action Plan 2021-2030: Towards Eliminating Avoidable Harm in Healthcare Care. https://www.who.int/publications/i/item/9789240032705
World Health Organization (WHO). (2023). World Patient Safety Day. https://www.who.int/campaigns/world-patient-safety-day/2023